D
deleted547631
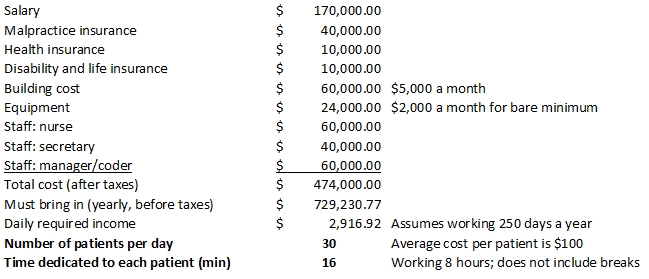
I'm interested to learn more about the income and business overhead numbers for direct primary care. Here's a scenario that I feel is what to expect based on numbers and percentages that I've read that are being bounced around. Assumptions: 100% accounts receivable. Overhead includes staff salaries (one LPN, one office scheduler and their benefits), medical malpractice insurance, office rent and utilities, equipment (computer and office EMR subscription), and medical supplies. Two weeks vacation (hence, 11.5 multiplier).
Average patient panel = 600 individuals
Average aggregate monthly charge per patient (range $40 - $79 per month depending on age for adults, $10 pediatric) = $60
Extra per month billing for house calls, additional procedures, profit on labs, etc = $1,000 (no reference for this figure)
Overhead percentage = 30%
([(600 * $60) + $1,000] * 11.5) * .7 = $297,850 net income after overhead
Are these numbers fairly close to what one could expect? Are overhead percentage and aggregate per subscriber monthly fee accurate? Please chime in! @AtlasMD
Average patient panel = 600 individuals
Average aggregate monthly charge per patient (range $40 - $79 per month depending on age for adults, $10 pediatric) = $60
Extra per month billing for house calls, additional procedures, profit on labs, etc = $1,000 (no reference for this figure)
Overhead percentage = 30%
([(600 * $60) + $1,000] * 11.5) * .7 = $297,850 net income after overhead
Are these numbers fairly close to what one could expect? Are overhead percentage and aggregate per subscriber monthly fee accurate? Please chime in! @AtlasMD


") options abound
options abound