- Joined
- Jan 31, 2009
- Messages
- 2,533
- Reaction score
- 206
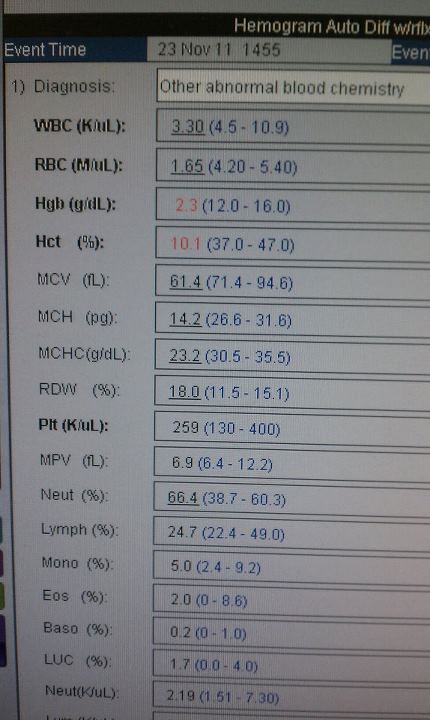
I had a patient come in with no significant history with chest pain & a troponin >220. She was 17.
Just out of curiosity, what made you order a trop on a 17yo with no significant history?

I had a patient come in with no significant history with chest pain & a troponin >220. She was 17.
Just out of curiosity, what made you order a trop on a 17yo with no significant history?
I was rotating at a peds tertiary referral center. The presentation was chest pain radiating to left upper extremity. Labs by committee.
What did the cath show?
ALL at 46? Dr. Goljan, you lie! That's pretty impressive though.
 No one can tell them anything. The cath lab NP comes in for the day and almost drops her cup of coffee when she sees the gas: pH 7.91, pCO2 13, pO2 412. We try to get them to give him some amiodarone (he's been shocked at least half a dozen times) but they need to "stabilize him" first. When he is perfusing for 5 minutes consecutively, I offer to take him (and try to get him somewhere safe) but they want to TPA him. Mind you, he's bleeding around his art line and central line sites, and has been on integrillin for 16 hours. Finally his cardiologist comes in takes control and sends me on my way. The guys on vaso, levo, neo and dopamine with a crap pressure. We get him to the receiving hospital and he never makes it to the OR.
No one can tell them anything. The cath lab NP comes in for the day and almost drops her cup of coffee when she sees the gas: pH 7.91, pCO2 13, pO2 412. We try to get them to give him some amiodarone (he's been shocked at least half a dozen times) but they need to "stabilize him" first. When he is perfusing for 5 minutes consecutively, I offer to take him (and try to get him somewhere safe) but they want to TPA him. Mind you, he's bleeding around his art line and central line sites, and has been on integrillin for 16 hours. Finally his cardiologist comes in takes control and sends me on my way. The guys on vaso, levo, neo and dopamine with a crap pressure. We get him to the receiving hospital and he never makes it to the OR. 
Gi upset x3 weeks. No PMD. Urgent care gave him Lomotil and started him on a PO anti-hypertensive for what he says was a BP of "240/120".
K+ 7, HCO3 11, Gap 31, BUN 159, Cr. 39.4 <- highest I've seen.
Ha! I think I slightly bettered this one today. Classic story for a PE. SOB s/p long transatlantic plane ride with leg swelling. Awake and talking, though shallow respirations. I STAT creatinine to get a quick CTA chest... >20.... Hmmm... recheck >20.
Labs:
Na 123
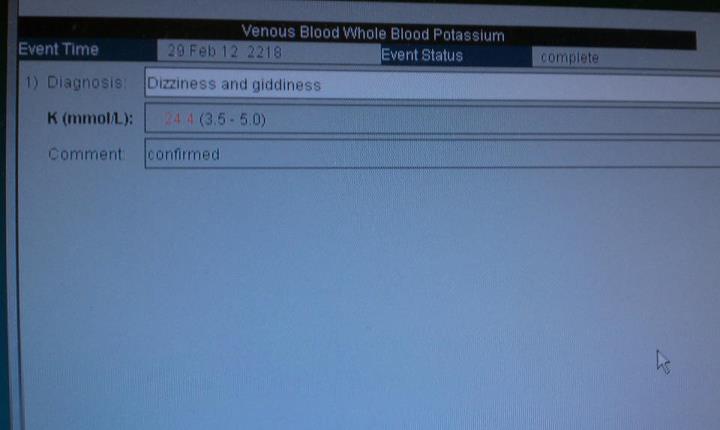
K 8
HCO3 7
Gap 32
Lactate 0.4
BUN 267 <-- by FAR the highest I've seen.
Cr 32
Definitely the worst BUN I've seen. I had one in the 180's a few months ago that I though was impressive, but that doesn't touch 267. damn.
Sodium of 99.
Awake and talking, although dyspneic from his entire right lung being whited out.
Cl- 57, K <2.0 (1.8 I think)
A 8 week kid whose (granted, uneducated but well meaning) parents had been taking him to the doctor for a few weeks because "all he does is throw up and get skinnier". Formula switched several times. Doctor unconcerned that baby 1 pound below birth weight. Parents hotlined for child neglect. Kid had pyloric stenosis.
Seeing a drunk today who's a regular. Looked it up in the system computer that covers 4 hospitals and he was in the ED 45 times in 2007. That's just my 4 houses, doesn't count all the other hospitals in town.
ED visits in 1 year = 45
Unerringly correct! I've never met an alcoholic with any other source of income.[/sarcasm]
ALL at 46? Dr. Goljan, you lie! That's pretty impressive though.
tonight my crushing chest pain patient, who said it was because her family made her take meth and cocaine....
K 10, Cr 21. pretty awesome ekg. baseline Cr a month earlier 1.3.
PEA arrest
Hg 1.7
LDH >27,000
LA 25
Acute drug-induced hemolytic anemia secondary to ampicillin infusion. Still alive.
Bmi 99.5
Bmi 99.5
Bmi 99.5

And DrMom: srsly? Did y'all have to use a crane to move that person to a stretcher? Would a stretcher work??
Fortunately they got to stay in their motorized WC.

Glucose: 1939
Sodium: 112... 156 after mdCalc's correction.
Guy's urine looked like syrup.
Ammonia 476. A little confused, yes.
Arterial pH 6.62
LOL came in altered and talking. Got dehydrated at home. Went into ARF with hyperkalemia. Didn't survive the night. Sad case.
Wow...Originally read LOL as "laughing out loud." Got to the end of the sentence and had to try again.