- Joined
- Jan 30, 2005
- Messages
- 2,752
- Reaction score
- 657

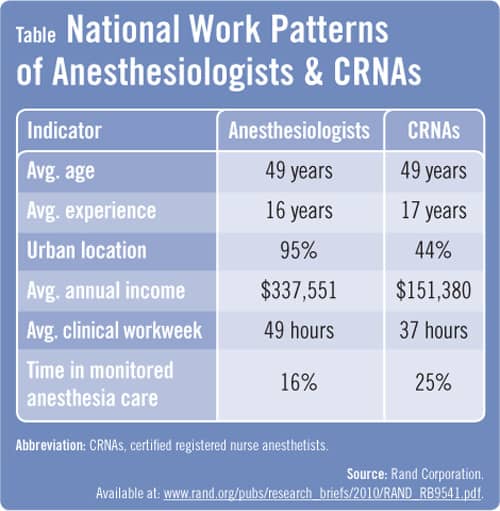
And the average weekly work hours are ~35 for CRNAs.

")
With the full assault by the AANA on this specialty the big wigs should be happy with this year's Match. The big pool of applicants seeking ANY Residency will keep the residency slots full. But, the competitiveness of the specialty is clearly on the decline.
cool, nice charts and stuff. but what do you recommend us to do? what are you personally doing about this nonsense?
[data not yet public]
Wow.
LOLHere is what you are Missing:
1. Ortho
2. Neurosurgery
3. ENT
4. Urology
5. Heme/Onc
6. Hand Surgery
7. Optho
8. Invasive Cards
Med Students need to look at all their options before choosing GAS.
We are approaching the era of "discount" medicine, like the airlines. How much did they pay the pilots 20 years ago? How much do they pay them now, on average? How did the public look at the pilots 20 years ago, vs now?To some extent, MD anesthesiologists have become a victim of their own excellence. Deaths during the administration of anesthesia occur at a paltry rate of 1/250,00 cases nowadays. This remarkable improvement can be attributed solely to technical improvements in the monitoring of patients during a procedure. Things like continuous pulse oximetry, end tidal CO2 monitoring, and fiberoptic-based intubation equipment have almost completely eliminated major morbidity from the profession. This is a good thing. But maybe not so good for anesthesiologists. They practice in a very algorithmic, checklist-based manner.
Thus, it was relatively easy to teach their methods to CRNA’s during a period when the exponential rise in operative case loads made it necessary to incorporate “anesthesiology assistants” into a practice, thereby allowing one attending physician to cover multiple rooms. That recent studies have confirmed what everyone else in the OR already knew—that it didn’t really matter who was behind the drape while a cholecystectomy was ongoing—- is hardly a surprise. The less variability in clinical excellence one sees from certain specialists, there seems to be a commensurate decrease in perceived prestige. In other words, one’s individual reputation as a doctor can be paradoxically harmed when the overall complication rate of your chosen specialty is so low. You are seen as a mere “cog in the machine”, a cog that could easily be interchangeable with another doctor or, in this case, a CRNA.
http://www.kevinmd.com/blog/2011/01/md-anesthesiologists-victims-excellence.html
He's counting his retirement money. He's just doing all of you a favor by warning you about what's coming.cool, nice charts and stuff. but what do you recommend us to do? what are you personally doing about this nonsense?
So some of you think midlevels wont replace EM docs but CRNAs can replace anesthesiologists? The last 3 times someone in my family ended up in the ER we saw a mid level provider until we were almost through the process and discharged. My EM buddies are more concerned than I am about being replaced. They also talk about management companies constantly. Our fields face similar threats, probably more alike than any other 2 specialties if you think about it. I'm not by any means suggesting we don't need docs in the ER. We do, as much as we need docs in the OR.
LOL
Sure didn't take long to get the obligatory "be brilliant and the world is your oyster" post.
Here's the thing Blade, a person who has the brains and drive to match into specialties like ortho, neurosurgery, ENT, and so on ... can surely be a top 10%'er in anesthesiology. While the overall job market for anesthesia isn't what it was 10 years ago, the top 10% are still doing very, very well.
80% or more of the people matching into anesthesia are not competitive for most of those specialties. Those specialties aren't options for them.
I've said this before, seems like a dozen times, when you post lists like this, you might as well be telling guys who are stuck playing minor league baseball that they simply should've chosen the NFL instead.
Study hard and outscore your peers on the STEP exam is hardly making the NFL roster. Top 1/3 of the med school class (M.D. USA) can still match into many great specialties.
Bottom 1/3 gets FP, Peds and soon Anesthesia.
Hence, I recommend you work your arse off in Med School so the world is oyster vs being a cog in the machine.
Not true at all schools. I know of some schools where many of the top applicants in the class (250+ step 1, AOA) match into fields like peds.
Please tell me if I am missing anything. With GAS, I can expect to pull in 400K, interesting phys/pharm/pathophys, ACLS skills, fun to be facile with procedures, privacy, no pt follow up. Americans will always demand high quality anesthesia care.
He's saying that if you are a bottom student, your options are limited. It's not a comment on what top students do or should choose
Not true at all schools. I know of some schools where many of the top applicants in the class (250+ step 1, AOA) match into fields like peds.
I don't understand why students on the bottom aren't all just becoming hospitalists (especially if you're willing to work nights for a few years or moonlight on your off weeks). Shift work and 250-300k+ doesn't sound like a bad deal when your step 1 is <=200.
Study hard and outscore your peers on the STEP exam is hardly making the NFL roster. Top 1/3 of the med school class (M.D. USA) can still match into many great specialties.
Bottom 1/3 gets FP, Peds and soon Anesthesia.
Hence, I recommend you work your arse off in Med School so the world is oyster vs being a cog in the machine.
That's not a bad option, but it's also becoming a saturated market. I suspect that will happen with EM as well 5-10 years from now, given the current boom and high interest from med students.
Actually, I'm not sure if top 1/3rd can match into the mostly sub-surgical specialties you listed. Maybe more like top 10-20%.Study hard and outscore your peers on the STEP exam is hardly making the NFL roster. Top 1/3 of the med school class (M.D. USA) can still match into many great specialties.
Bottom 1/3 gets FP, Peds and soon Anesthesia.
Hence, I recommend you work your arse off in Med School so the world is oyster vs being a cog in the machine.
Study hard and outscore your peers on the STEP exam is hardly making the NFL roster. Top 1/3 of the med school class (M.D. USA) can still match into many great specialties.
Bottom 1/3 gets FP, Peds and soon Anesthesia.
Hence, I recommend you work your arse off in Med School so the world is oyster vs being a cog in the machine.
We agree, be brilliant and work hard and things will go well for you.
My point, perhaps not clearly stated, is that the kind of top 10% med students who have the option of matching into your list of highly competitive specialties are also the kind of people who, if they choose anesthesia, are going to wind up in the top 10% of anesthesia jobs, and that ain't bad.
These people will be chief residents at top tier programs and will network into great jobs.
These people will do fellowships at top tier programs and will network into great jobs.
The problem with your advice, is that the cohort that can actually take it, doesn't need it, because they're going to excel in whatever field they choose. Even anesthesiology.
What are your thoughts about going into anesthesia if an applicant is competitive enough to match into a well-ranked (e.g. top 25) major academic program in anesthesiology? (assuming he/she doesn't want to do other fields)
I don't even know if top 10% means much when it comes to landing a high paying anesthesia job. I think it's almost always who you know. If you look at gas work and cold call, you will think the job market sucks. One of the most competitive groups where I did my fellowship hired one of the residents from my program and he was terrible but he knew somebody over there. One of my co fellows applied and didn't even get an interview and he was really strong, good personality, good scores.
That's my point. Anesthesia is a "roll of the dice" when it comes to landing a top 10% type of job. It comes down to "who you know" rather than "what you know" to get one of these jobs.
This is the reason I would recommend a bottom 10 ORTHO Residency over a top 10 Anesthesiology Residency. The odds heavily favor the fact the Ortho graduate will be able to secure a very nice gig after training since the Median salary is so much higher than GAS.
Of course, a med student needs to pick the specialty which he/she can see doing for the next 30 years. Those with options really need to choose wisely.
So only derm, surg subs, gen surg, and a ballooning bull market EM had more US Grads matching than Anesthesia. But you all still say its on decline? Anesthesia is still moderately competitive. Just has been recently overtaken by EM which has much more spots. Wouldn't be surprised to see that bubble burst in 5 yrs or so.
So only derm, surg subs, gen surg, and a ballooning bull market EM had more US Grads matching than Anesthesia. But you all still say its on decline? Anesthesia is still moderately competitive. Just has been recently overtaken by EM which has much more spots. Wouldn't be surprised to see that bubble burst in 5 yrs or so.
That's an odd result IMO, they are really low hanging fruit for midlevels.
I agree. EM has become so protocol based. PA's and NP's can work the room easily. Plus insurance companies are doing everything possible to reduce annual ER visits and re-route patients to PCP. While the revers is true for surgery. This bodes well for anesthesia
You mean it bodes well for CRNAs.I agree. EM has become so protocol based. PA's and NP's can work the room easily. Plus insurance companies are doing everything possible to reduce annual ER visits and re-route patients to PCP. While the revers is true for surgery. This bodes well for anesthesia
Who has more pull/power in hospital politics, interventional/ep cards or surg subs?
You mean it bodes well for CRNAs.
Who has more pull/power in hospital politics, interventional/ep cards or surg subs?

So only derm, surg subs, gen surg, and a ballooning bull market EM had more US Grads matching than Anesthesia. But you all still say its on decline? Anesthesia is still moderately competitive. Just has been recently overtaken by EM which has much more spots. Wouldn't be surprised to see that bubble burst in 5 yrs or so.
How is anesthesia moderately competitive? I consider EM and gen surg as moderately competitive. Anesthesia is the hardly above family or internal.
They'll certainly get a share of the pie just as any other MidLevel. Probably more so in rural areas. Call me optimistic but as someone who matched Anesthesia yesterday, I'm more than satisfied with my specialty choice even if it means tacking on an extra 12 months doing a fellowship to gain more job opps
Congrats on your match. You're still very early in the game. PGY 1 is nothing like residency which is nothing like being an attending. Take what you read on here with a grain of salt, but at the same time, read closely to what people who have been in the game long are saying. They could give you some good advice.
If you like pain, do that fellowship and buy into a surgery center. I seriously considered this and love the procedures but just can't tolerate the patient population. I'd have been a miserable SOB for the rest of my career.They'll certainly get a share of the pie just as any other MidLevel. Probably more so in rural areas. Call me optimistic but as someone who matched Anesthesia yesterday, I'm more than satisfied with my specialty choice even if it means tacking on an extra 12 months doing a fellowship to gain more job opps
If you like pain, do that fellowship and buy into a surgery center. I seriously considered this and love the procedures but just can't tolerate the patient population. I'd have been a miserable SOB for the rest of my career.