So you want a race to the bottom with CRNAs? Even if we win, we lose. Big time. The only winners are the organizations employing the competing suckers.
The only solution is decreasing the number of residency grads, so that anesthesiologists will remain highly sought after. Which ain't happening. Ergo, any smart student shouldn't touch anesthesiology with a pole. Knowing what I know now, I wouldn't. And I am sorry I have to say this, but if one doesn't see any better specialty fit or path, then maybe one shouldn't be in medical school in the first place.
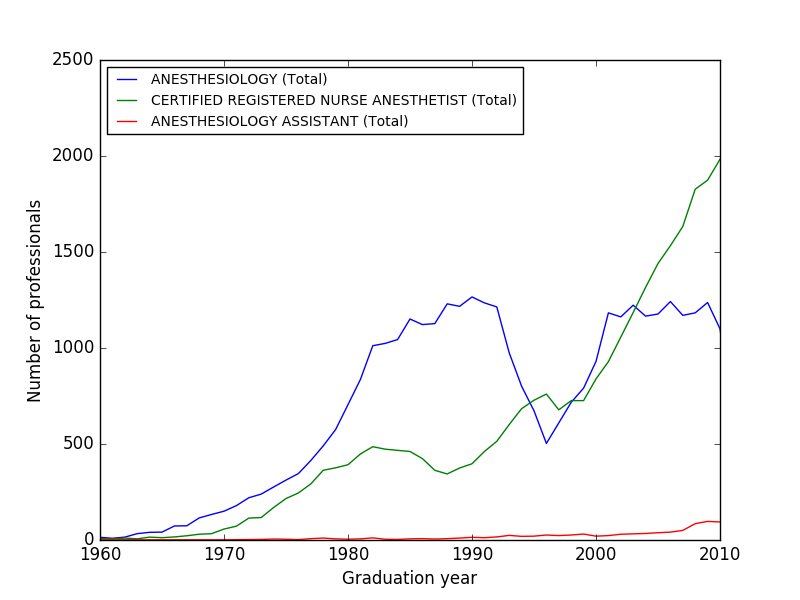
If you think a fellowship will protect you, think again. Unless that fellowship requires a good amount of physician-level judgment, it won't. First step for the AANA is independence, second step is going for anything that is highly productive and protocoled (community cardiac comes to mind, especially if there is a cardiologist who does the TEEs). There is already an overproduction of CRNAs, and not enough easy patients/procedures. (There is also an overproduction of anesthesiologists, for most markets, by the way.) Physicians will be the firefighters, covering more and more rooms at a time, and/or will work at a fraction of today's incomes, and/or will move to BFE (or wherever noone wants to go, or do what noone wants to do, to maintain a higher income than CRNAs). Yes, patients will suffer more harm with nurse coverage, but healthcare organizations only care about their bottom line (and definitely not about your future malpractice history, career or job satisfaction). This won't happen overnight, but faster than you think. Even just 5 years is a long time in anesthesia nowadays. (Heck, it was only about 10 years ago when I decided to go into anesthesia.)
Tl;dr: if you want anesthesia, go become a CRNA, or AA, don't waste your time and money with medical school.
")