
- Joined
- Oct 18, 2004
- Messages
- 391
- Reaction score
- 29
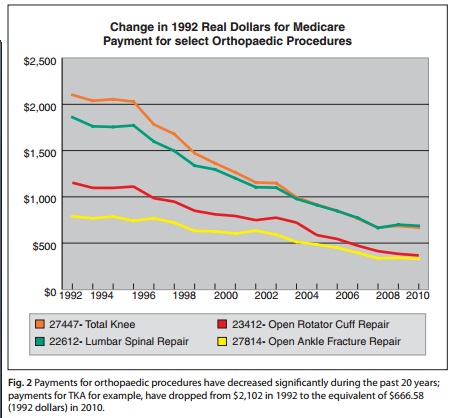
Sobering article from the AAOS on Medicare reimbursement cuts to orthopaedics. Rumors are there will be more Medicare cuts to ortho in 2013, with private insurers to follow.
http://www.aaos.org/news/aaosnow/dec12/cover1.asp
And from Orthopedics Today:
http://www.aaos.org/news/aaosnow/dec12/cover1.asp
And from Orthopedics Today:
Fehring: While our group may allow senior partners to drop Medicare, our hip and knee center has decided not to pursue this strategy. While this approach may be financially advantageous for a senior partner, we must not allow unreasonable governmental reimbursement cuts to further divide our orthopedic groups and subspecialties. Opting out of Medicare would cause significant dissention within our group. It would significantly limit the earning potential of the younger physicians who would bear an inordinate load of Medicare and Medicaid patients.
We feel it is the obligation of all members of our group to service all of the patients in our community who need hip and knee replacement. We need a solution that helps all arthroplasty surgeons, not just a select few.
Scully: Nothing would happen if senior surgeons resigned from Medicare. If 25% or more of all surgeons refused Medicare patients, that might get noticed. But there is very little sympathy for surgeons in Washington. There is far more compassion for nurses, general practitioners (GPs), emergency room physicians and others. This may not be fair given the massive loss of surgical income in the last decade, but that is the reality.
Lavernia: How low would the primary reimbursement have to go until significant numbers of hip and knee surgeons stop taking Medicare patients?
Fehring: I think we are very close to that level. Since 1990, the reimbursement for hip and knee replacement has gone down 64% and 59%, respectively, in inflation-adjusted dollars. We have allowed the government to perform what I term a "boiling frog technique" with regard to hip and knee replacement reimbursement. If you put a frog in a pot of water and raise the temperature slowly, the frog acclimates. But if you turn the heat up 100° and throw the frog in, he would jump out quickly.
Medicare has decided to slowly ratchet down the reimbursement for hip and knee replacement to lower costs, yet keep physicians in the pot. With each decrease, we pedal harder to maintain the same income. Eventually, you can only pedal so fast before you burn out.
I think we are rapidly reaching the point where we can not squeeze out any more efficiencies from our system or do more cases daily. If cuts continue, eventually the overhead expenses will become similar to the reimbursement. This will be intolerable and will force most dedicated hip and knee surgeons to drop Medicare.
Attachments

Last edited: