- Joined
- Sep 28, 2009
- Messages
- 124
- Reaction score
- 13
Some interesting statistics and facts about the number of anesthesiologists, the population, and other anesthesia providers....
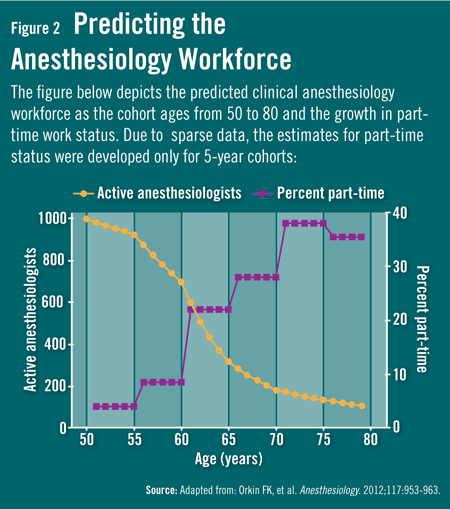
Also, given that there are around 45,000 practicing anesthesiologists and about 1,600 new anesthesiology resident graduates per year, what does this say about future numbers? If the average career lifespan of an anesthesiologist is 35 years (estimate), this means we only need around 1,300 anesthesiologists per year to preserve the current workforce. Is the aging population and population growth enough to offset the ~300 increase in the anesthesiologist workforce per year?
- In 2012, there were 45,357 anesthesiologists. This represented 5.8% of all physicians in patient care activity in 2012. This is up from 39,032 anesthesiologists in the workforce in 2003.
- Between 2003 and 2012, the physician anesthesiologist workforce increased 16.2% over this 10 year period compared to a 13.4% increase in the overall physician workforce.
- Using Medicare 5 percent beneficiary sample claims data, the number of physician anesthesiologists and nurse anesthetists with Medicare claims between 2009 and 2012 was examined. Over this time period, the number of nurse anesthetists increased almost 3x faster (14.7%) than the number of anesthesiologists (4.4%).
- Between 2001 and 2011, the number of graduating nurse anesthetists more than doubled (from 1,159 to 2,447).
- The ratio of the number of anesthesiologists to population between 2003 and 2012 grew 7.4%.
- Changes in the number of gastroenterologists and in the number of surgeons within a state had a relatively large and significant effect on the number of anesthesiologists. This accounts for 95% of the variation of change in the number of anesthesiologists across states.
- Finally, there is no significant correlation between CRNA-supervision opt-out states and the change in anesthesiologists per population ratio for states. (That is to say, there are some opt-out states which had a decrease in this ratio, and others which had 10-20% increases).
- An update to the RAND Corporation report in 2010 will be forthcoming later this year (anesthesiology workforce survey and analysis report).
Also, given that there are around 45,000 practicing anesthesiologists and about 1,600 new anesthesiology resident graduates per year, what does this say about future numbers? If the average career lifespan of an anesthesiologist is 35 years (estimate), this means we only need around 1,300 anesthesiologists per year to preserve the current workforce. Is the aging population and population growth enough to offset the ~300 increase in the anesthesiologist workforce per year?