It's Not Just In Your Head
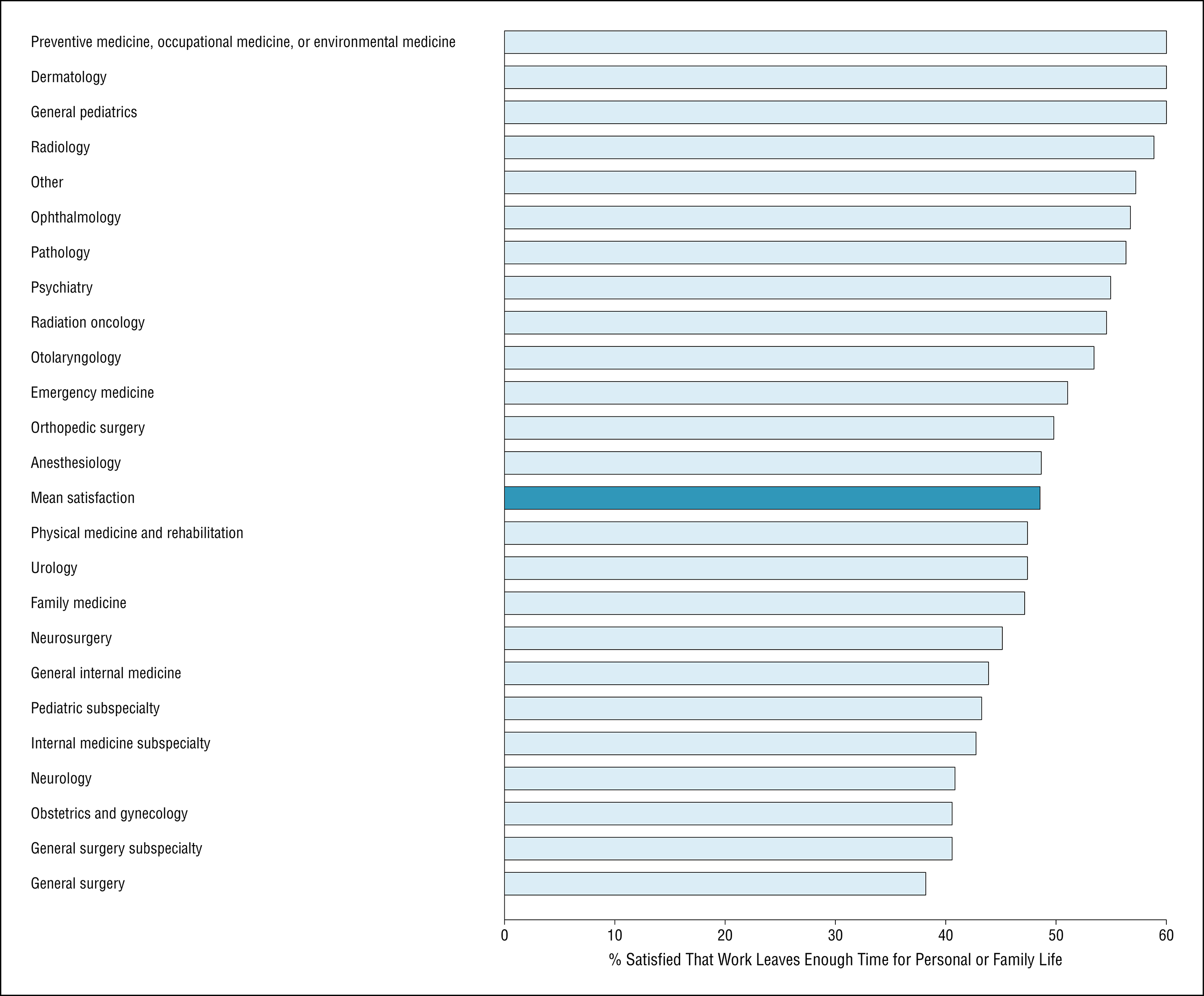
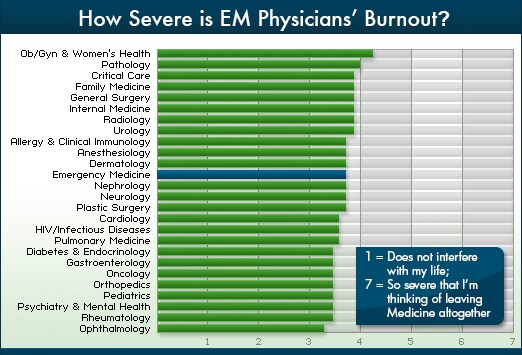
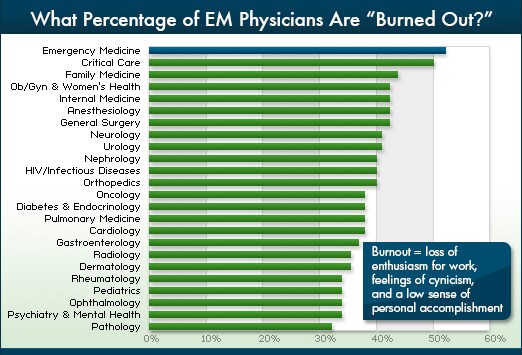
I'm glad you love your version of Emergency Medicine, EmergentMD. I also love my very non-traditional, sub-specialty version of Emergency Medicine, that I've carved out for myself through extra training, extra work, time investment and additional sacrifice. I wouldn't describe myself currently as feeling "burned out" at all, but I've been there. And with all due respect, this post seems to me like the classic, "Suck it up. Get over it. You're imagining it. The problem is you," response to burnout in Emergency Medicine. I've been hearing various responses like this, since my years as a medical student, through residency, and it continues now in my years as an attending. The guy who got burned out, "Was weak. He had a midlife crisis. Or he just was chronically unhappy," or just needs to move and find a new job. It's the same old story, with various responses explaining the problem away, rather than addressing it's causes and solutions. Yet the survey's still show, that not only does Emergency Medicine consistently rank #1 out of specialties of physicians reporting burnout, in multiple surveys (
Medscape survey, slide 2;
JAMA, figure 1), but the proportion tends to be over 50%. In other words, if you
don't report feeling of burnout, defined as "loss of enthusiasm for work, feelings of cynicism, and a low sense of personal accomplishment," then
you are actually the weird one.
I don't think any Emergency Residents or Physicians really, truly expect or demand to see "only really sick patients," as you claim. I don't know one Emergency Physician, that didn't know he'd be doing a lot of primary care. But your example of managing 5 crashing patients, leaves out one very, very large 900 lb gorilla in the room, doesn't it? The 900 lb gorilla in the room is the fact, that many ED directors, most of whom take their marching orders from the non-physician administrators of hospitals for higher pay and less clinical shifts, will still expect the 25 non-emergencies in the waiting room to be "greeted," "door-to-roomed," "arrival-to-physician'd" in some outrageous, unrealistic, unnecessary and impossible time goal, that a physician working a max capacity has no control over. I can honestly say, that just about every Emergency Physician I've ever known, if expected to manage 5 critical patients, would say, "Bring it on, baby," and high-five his partner who comes on a 7 am shift change when telling how he got through it. Certainly, most would not want
every shift to go that way, but I don't know one that would "cry in the corner" over it, as you claim. But I've never know one single Emergency Physician, that ever felt he or she deserved to be told, directly or by implication, that he "sucked" if the 25 non-emergencies in the wait room weren't "greeted" or "roomed" or in some other way put in a box with a bow wrapped around them, while his head spun manging the five patients circling the drain of life.
So, I find it very interesting, and pertinent that you are or have been, an ED director for the majority of your 15 years. I find that
very interesting, and telling, as ED directors typical work far less shifts, make the schedule and generally have as much or as little exposure to the trials and tribulations of the "pit doc" as they choose. I also find it very interesting that you made the point to write a post about how happy you were with your job, yet didn't really seem to offer anything that would allow those that described having trouble in their situations other that to seem to imply that all that is needed is for them to snap out of it, by realizing someone else has it worse, and if unable, they are flawed. That may work for some people, but it's not particularly helpful for some, because there's
always someone with it "worse." Nobody wants to be "just a little bit better than '
worse.'" Some may want their job to make them happy, but I think most of all Emergency Physicians just want to be appreciated. And they don't want to be told they suck because a hang-nail waited and hour while they did manage 5 crashing patients. I've had many shifts, single coverage where I managed 5 crashing patients, as I'm sure you have over the years. I've had 12 beds full, with several sick and intubated and had a rollover MVA come in with 4 patients ejected, all on backboards covered in blood, with help no sooner than 30 minutes away,
if I could get help on the phone and on their way in.
That's all stressful, and you know that. We all signed up for "stress." It's numbers one, two and three in the job description. But none of that was what changed things for me, personally. None of the emergencies, nor any of patients who came in with hang nails, work notes, earaches or med refills changed anything for me. I always welcomed the easy patients as a break between real emergencies. But what did it for me, and what made me realize I was fighting a futile and losing battle every day, was that despite the heroics, the shifts I didn't think I could handle but did, the chaos I didn't think I could bring under control but did...it was never good enough.
It was never good enough.
I came to the realization, that I could save a life, 2 lives, or three in a shift, and I could be told the next day that it wasn't good enough because the "hang nails" waited on average, 2-minutes longer than "corporate" wanted. And it never came as bluntly, or as direct as, "You suck." It always was dressed in pleasantries, cloaked with buzzwords like "patient satisfaction," "efficiency," and "administration," which I took on face value for a long time. The closing line was always the equivalent of, "Do the impossible, or you'll lose your contract." It's about nothing more than money. It has nothing to do with "healthcare," a "crisis," or "the sick." It's about maximizing flow,
specifically of the "unsick" through the ED to make maximal profits for the hospital CEO, and/or shareholders, and/or to go into the not-for-profit hospital's kitty for next years administrator's salary increases. The more the billboard can push down the street to the ED, the better, with no limit. It took me quite a long time to learn the language and translate the message. And now, I thank God every day, that I don't have to go through the passive aggressive manipulation anymore, and have an ED director tell me it's all in my head. I am also equally as thankful, that I found a way that I can use my skills as an Emergency Physician without starting over, and was able to build on them in a way that I'm able to have much more control over my practice life, hours, and future.
So, did I have it "good compared to the general population"? Absolutely. Do I have it even better now, that I made some drastic changes? Yes. Do the 50-70% of Emergency Physicians who report burnout feel exactly the same way I did, or have the same exact experiences I did? Likely not. But there something there.
It's. Not. Just. In. Their. Heads.
They're not lying in those surveys. They're not "chronic complainers," "wimps," or having delusions of failure. Neither are any of the tough, hard-nosed, heroes on this thread or those in Emergency Departments across this country that have dedicated their lives to working on the front lines of the chaos that is Amercian Emergency Departments today. Despite the high salaries, the supposed "great hours," and despite the reports from those who just don't see what all the fuss is and think the rest need to just "suck it up," there's something there. So just keep telling the bright-eyed bushy-tailed hopefuls that its just a bunch of BS, that there's too many complainers out there that need to step aside and get out of the way. And do nothing to solve the problem, for those that signed up to go to battle with you, and for you.
Slide 2:
http://www.medscape.com/features/slideshow/lifestyle/2013/emergency-medicine#2
Figure 1:
http://archinte.jamanetwork.com/article.aspx?articleid=1351351