
- Joined
- Jan 18, 2008
- Messages
- 12,729
- Reaction score
- 4,899
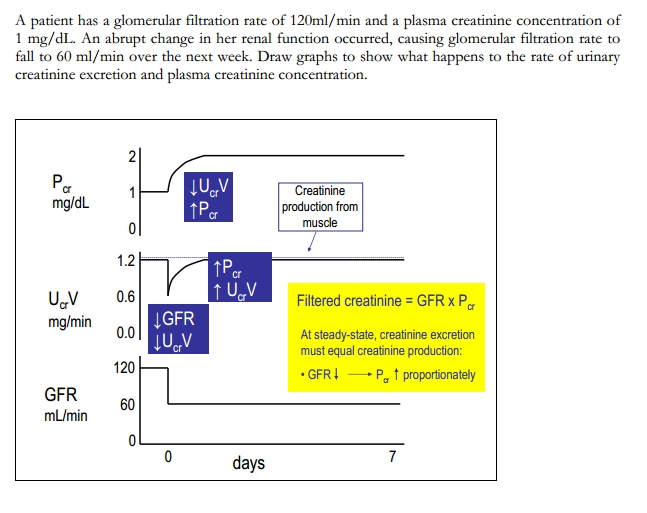
I want to know what equation to use in figuring out the answer. Assuming a 125 GFR being reduced to 20% (25) doesn't begin to explain the excreted creatinine. Or my professor never explained chronic renal failure's influence on excreted creatinine. I understand the levels of plasma creatinine increasing but not the levels of creatinine in the urine remaining the same and not substantially reducing. Is there a formula I'm missing here?

")