
- Joined
- Nov 13, 2017
- Messages
- 39
- Reaction score
- 12
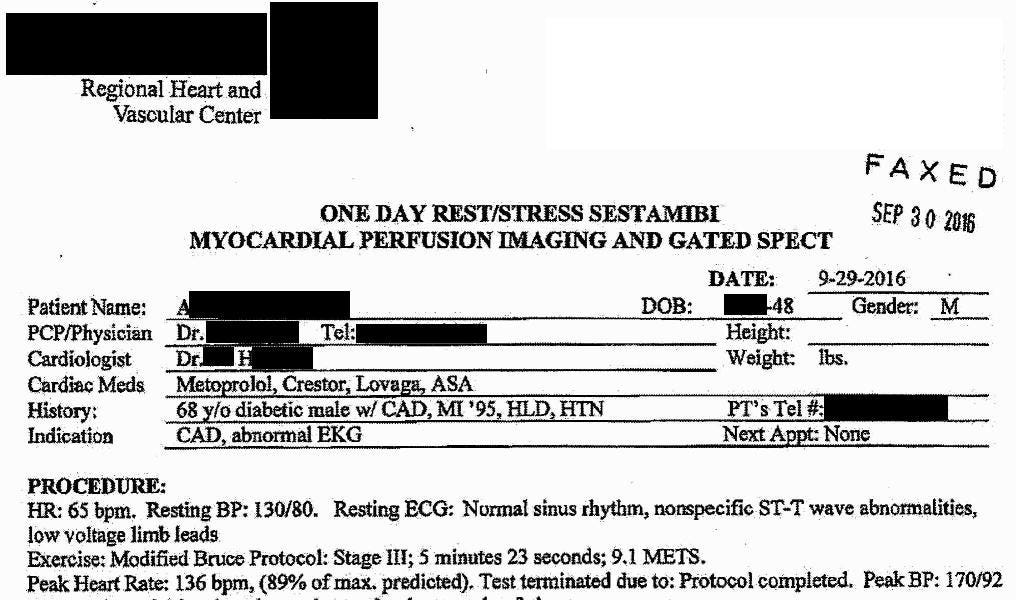
Expert Witness Case #2
This case concerns a 68-year-old man, referred to as Mr. A. He had a history of previous myocardial infarction and was cared for by his primary care doctor. After a long period of limited follow-up, his PCP encouraged him to see his cardiologist (Dr. H) after noting “more prominent ST-T wave...
 expertwitness.substack.com
expertwitness.substack.com
68-year-old man with history of MI seen by nurse practitioner.
Stress test ordered.
Results show ischemia, but no one communicates with each other about it.
I'll let you guess what happens while he is playing golf a week later....