- Joined
- Jan 2, 2014
- Messages
- 11,384
- Reaction score
- 24,014
it's hard to donate to a group that doesn't stand up for you, trumpets horrible ideas and wastes money on a fancy, brand new headquarters

Yeah, i get emails from the ama congratulating me on the aca....it's hard to donate to a group that doesn't stand up for you, trumpets horrible ideas and wastes money on a fancy, brand new headquarters
The government funding things is precisely why PCPs will always be paid less. There's simply more of them, and we can't afford to give them all neurosurgeon levels of pay.
More likely they'll bring everyone down, not just the top. The goal of turning physicians into employees is already in full swing in nearly every specialty. Once that's compete, they start tightening the screws. Right now that's politically untenable, because they'd be cutting doctor's pay directly. With bundled payments, however, they can claim they're cutting payments to the greedy hospitals, who will in turn cut the salaries of physicians. The politicians are absolving themselves of the political consequences by using bundled payments to obfuscate what's actually happening.With the current climate the general movement is to bring the top down, not bring the bottom up.
In 5 years the median pay will be lower, much fewer true private practice jobs and more supervision of crnas (3-5 crnas per MD). AANA will use the ACA to keep chipping away at independent practice. A good analogy is a prisoner trying to dig his way out using a spoon. Progress is measured in decades not days.
Lol, you have no idea what you are talking about. Where is this "glut" of physicians going into primary care? Not sure where you are getting your information, but primary care, EM, and psych are easily the best job markets in all of medicine right now. I literally get inundated with PCP offers on a daily basis (have to start blocking recruiters), and offers are going up because health care organizations don't have ENOUGH primary care - not too much. Obviously, the market in large cities are a bit more saturated, but what field isn't? Everyone in IM is going into hospital medicine or sub-specialty. There were maybe 2 ppl in my class of 50 that went into outpatient general medicine. And FM itself isn't enough to fill up the PCP need in this country.More likely they'll bring everyone down, not just the top. The goal of turning physicians into employees is already in full swing in nearly every specialty. Once that's compete, they start tightening the screws. Right now that's politically untenable, because they'd be cutting doctor's pay directly. With bundled payments, however, they can claim they're cutting payments to the greedy hospitals, who will in turn cut the salaries of physicians. The politicians are absolving themselves of the political consequences by using bundled payments to obfuscate what's actually happening.
EMR wasn't about patient safety or cost savings. It was about increasing overhead enough to force physicians to become employees. Same goes for all the new regulations that came along with Obama's mess of a law. I guys what I'm saying is that the future isn't bright wherever you look. Anesthesia is certainly no exception. But with the glut of providers going into primary care and the majority of PCPs now in large groups or bring employees by hospitals, they'll probably see the bottom fall out before anesthesia, particularly with the necessity of anesthesia in cash cow surgery procedures versus the money drain that is primary care.
Can somebody explain why Anesthesiologists are making the choice to be employed rather than own their own practice? What economic pressure is driving all these docs to sell out? Are specialties that don't rely on the hospital, like FM, psych, ever going to face these pressures?
Its all about money plain and simple.
Imagine you are a senior partner at a independent anesthesia group. You and your other senior partners have a few years left till retirement, say less than 5. All the sudden a big AMC approaches your group and says we will buy your group out of its current contract with the hospital for $2 million per partner. In addition you all can work as employees for us with full benefits for as long as you want until retirement. Sure you have partners in your group who are still young and not far out of residency with 30+ more years to practice but you and your senior partner buddies have controlling voting rights within the group.
What would you do?
But the younger docs could start their own practices if they wanted to.
1/4 of us are earning record profits as well.This fact is best shown in the trending of academic salaries. If things are so rosy out there why does academic pay keep declining in your chart? Is it because there is a glut of labor for the Chairs to squeeze extra hard?
NPs can't do everything like a doctor, but they can lobby for permission to claim they are equal. You are welcome to claim your english bulldog can outrun a cheetah, doesn't make it true.And if NPs can do everything a FM doc can, why is there such a need for FM docs? Seems society values the extended training and knowledge of physicians somewhat, OR they just need someone to "supervise" FM NPs in states where they can't practice independently.
NPs can't do everything like a doctor, but they can lobby for permission to claim they are equal. You are welcome to claim your english bulldog can outrun a cheetah, doesn't make it true.
NPs can't do everything like a doctor, but they can lobby for permission to claim they are equal. You are welcome to claim your english bulldog can outrun a cheetah, doesn't make it true.
Well, for starters, the docs can have a much better understanding of disease process, greater ability to conduct a physical examination, interpret labs and other tests, have a higher intelligence to put all the data together and come to a diagnosis.
Sent from my iPad using Tapatalk
Yes.So doctors are just overall smarter?
Yes.
I can play football, doesn't mean I come close to Tom Brady. Not sure why that's a difficult concept.

Hey,
So I started my primary care gig with kaiser after residency. About 7 years ago this kaiser region was seeing red and about to go under. They brought in consultants (ie Bain/McKinsey types) to see how they could save money, provide good care and stop hemorrhaging patients. One of the first things they did was take NPs out of primary care. They took away their panels and made it MD/DO only. They transferred them into specialties were they did well defined procedures and types of visits. Ie go to ortho and do joint injections
More knowledgeable, smarter, more cost effective, all of the above? idk what it was but they have not looked back. The physician only primary care model has worked. The change has worked. With the realms of data kaiser collects they probably have the data to prove it but can't publish it to be PC.
I'll tell you another thing. They are desperate for primary care doctors and they are willing to pay for them. They will not go back to the old model . I know you guys may smirk at these figures. But if you told me 5 years ago that 240k base plus bonus/pension/5% match with no call and no weekends 800-500pm was possible in FM I would have laughed. That's the reality and they still can't get adequate staffing. When direct primary care takes off it will only get worse. Well I guess better
..Is it normal that cRNAs have access to the doctor's lounge? Just wondering, because at my hospital they do.
Just wanted to add. If buyout for younger docs is high enough (2 plus million per partner) taxed at 15-20% rate.Its all about money plain and simple.
Imagine you are a senior partner at a independent anesthesia group. You and your other senior partners have a few years left till retirement, say less than 5. All the sudden a big AMC approaches your group and says we will buy your group out of its current contract with the hospital for $2 million per partner. In addition you all can work as employees for us with full benefits for as long as you want until retirement. Sure you have partners in your group who are still young and not far out of residency with 30+ more years to practice but you and your senior partner buddies have controlling voting rights within the group.
What would you do?
Just wanted to add. If buyout for younger docs is high enough (2 plus million per partner) taxed at 15-20% rate.
You could bet set for life even with a 2 million buyout at age 40.
Unless you are simply careless with your money. Most of us (my cohort) in late 30s/early 40s should have net worth between 750k-1.5 million (that's just average) from working the past 10 year. That's already accounting for housing losses (for those of us who brought at peak and took losses) and stock market crash and recovery.
Money generates quickly once u get over 1 million. And that's with even conservative investing.
So add another 1-1.4 million post tax buyout money to your already net worth even at age 40. You are talking now having 2-2.5 million.
Sure you will be working simply cause you are able body and the money is still there even as employee. But once you reach a certain mark. You are pretty much set for life even investing conservatively.
So it's not only the old guys selling but younger guys can get a jump start on inching closer to retirement.
Blade, why is it that so many qualified US MD grads, who score >240s of the USMLEs still go into a dying specialty like anesthesia?
also, how easy would it be to switch to primary care ie FM, IM from anesthesia? Does it even occur that often?
cause not everyone choose career based on money? i chose anesthesia b/c i couldn't see myself doing social work all day on medicine, or round 5 hours. I didn't wan to stand in one spot for a big part of my day in surgery. It was either radiology or anesthesiology, and neither are doing well
Rads= Interventional
Anesthesiology= Peds, Cardiac, Critical Care or Pain
That's how I see it going forward.
By 2015 the DNAP CRNA should be in place for some schools. I suspect the Obama Health Care plan will be in full swing as well.
My conjecture is that MD Anesthesiology income is reduced 25-30% from today's levels. CRNA income should hold at today's levels but I am not sure if cost of living is keeping up with the dollar now known as hard toilet paper.
Anyone else care to speculate?
Swing and a miss.
Been 7 years and anesthesia is still a great gig.
But wasn't that the whole point of the thread?It's easy to say someone is wrong after the fact.
Swing and a miss.
Been 7 years and anesthesia is still a great gig.
7 years ago there were thousands more partnership jobs than there are today.
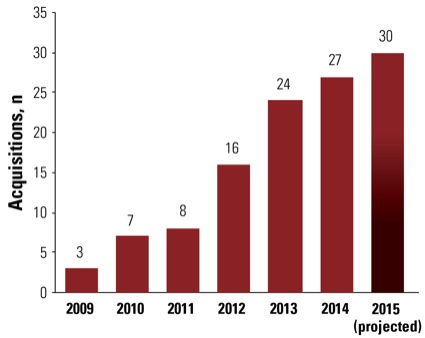
Take a look at this graph since 2009 and tell me things haven't changed significantly:
Hey,
So I started my primary care gig with kaiser after residency. About 7 years ago this kaiser region was seeing red and about to go under. They brought in consultants (ie Bain/McKinsey types) to see how they could save money, provide good care and stop hemorrhaging patients. One of the first things they did was take NPs out of primary care. They took away their panels and made it MD/DO only. They transferred them into specialties were they did well defined procedures and types of visits. Ie go to ortho and do joint injections
More knowledgeable, smarter, more cost effective, all of the above? idk what it was but they have not looked back. The physician only primary care model has worked. The change has worked. With the realms of data kaiser collects they probably have the data to prove it but can't publish it to be PC.
I'll tell you another thing. They are desperate for primary care doctors and they are willing to pay for them. They will not go back to the old model . I know you guys may smirk at these figures. But if you told me 5 years ago that 240k base plus bonus/pension/5% match with no call and no weekends 800-500pm was possible in FM I would have laughed. That's the reality and they still can't get adequate staffing. When direct primary care takes off it will only get worse. Well I guess better
It's easy to say someone is wrong after the fact.
