- Joined
- Nov 23, 2012
- Messages
- 692
- Reaction score
- 322
Starting salary for Gas is only 20K more than a 9-5 clinic gig w/ no emergencies (Rheum)

Starting salary for Gas is only 20K more than a 9-5 clinic gig w/ no emergencies (Rheum)
") )
)I chose to post first year out data in an attempt to better reflect what new graduates are earning.No. Those numbers are misleading. You can work 0700-1600 5 days a week with no call and earn that $240-$250K number. You may start at $250K but in 2-3 years the real number is $360K in 2016 which was $450K in 2009 (private practice). Of course, you will work 50 hours per week to earn that money.
Why look at FIRST YEAR OUT? look at 3 years out to get a better picture or even 5 years out.
Again, the truth is rarely posted online (except of course right here
Starting salary for Gas is only 20K more than a 9-5 clinic gig w/ no emergencies (Rheum)
If anesthesia generates the revenue it does per MD, how exactly is it a money loser for hospitals? Are the hospitals just not playing their cards correctly?
https://www.staffcare.com/uploadedFiles/2015-compilation-of-physician-compensation-surveys.pdf
Better data for you to use.
Merritt Hawkins’ numbers therefore are indicative of starting salaries. Merritt Hawkins’ numbers include only the salary or income guarantee amount and are not inclusive of production bonuses or benefits.
Although (ouch) according to Merritt Hawkins noninvasive cards is $291,000 (-34.2%)! I assume that lumps in a bunch of different cards subspecialties though including general.Thanks for that pdf, very useful!! Wow i should have thought harder about gastroenterology and cards.
https://students-residents.aamc.org/financial-aid/article/starting-salaries-physicians/
Starting Salaries for Physicians
Information obtained from the MGMA 2015 Physician Placement Starting Salary Report. The report is based on 2014 survey data for first year post residency or fellowship compensation.
Specialty Median
Anesthesiology $242,625
Cardiology: Electrophysiology $280,000
Cardiology: Inv-Intvl $437,500
Cardiology: Noninvasive $378,000
Dermatology $325,000
Emergency Medicine $275,000
Endocrinology/Metabolism $200,000
Family Practice (w/OB) $187,298
Gastroenterology $337,500
Hematology/Oncology $325,000
Hospitalist: Internal Medicine $205,378
Infectious Disease $185,000
Internal Medicine: General $180,000
Nephrology $180,000
Neurology $250,000
OB/GYN: General $232,500
Ophthalmology $180,000
Ortho Surgery: General $400,000
Ortho Surgery: Hand $330,000
Ortho Surg: Sports Med $325,000
Otorhinolaryngology $332,500
Pediatrics: General $160,000
Physiatry (Phys Med & Rehab) $195,000
Psychiatry: General $185,300
Pulmonary Medicine: General $305,000
Pulmonary Medicine: Critical Care $325,000
Radiology: Interventional $340,000
Radiology: Diagnostic $285,000
Rheumatology $221,000
Surgery: General $327,500
Surgery: Neurological $475,000
Urology $324,270
Reprinted with permission from the Medical Group Management Association.
If anesthesia generates the revenue it does per MD, how exactly is it a money loser for hospitals? Are the hospitals just not playing their cards correctly?
One of my personal thoughts (without a ton of administrative experience). Think of it this way. (Assuming all MD model for simplicity but ACT model would work too.)
Hospital with 2 ORs. Between vacation, sick/leave, post call, etc., you probably need 3 anesthesiologists to reliably cover. Making 300K/pop, that's 1.2 million/year, or $450,000/OR/year for anesthesia. If you want to make dead certain you can cover you hire 4 and now you're looking at $600,000/OR day for anesthesia/year. You never know with leadership roles and meetings etc.
Bigger hospital with 10 ORs/day, between vacation sick/leave, post cal, etc, you probably need 13-14 anesthesiologists. Now you are looking at some good vacation time and about $390,000/OR/year for anesthesia.
Bottom line: There is strength in numbers. You can run the same amount of ORs at less money with a bigger group. So you get a bigger group by finding a larger private group/AMC who can shift people around hospital to hospital and make things work. Have them sign a contract saying that they will show up when a case is posted, and voila, they will save more money if for no other reason that they are staffing the ORs consistently with just the right amount of people they need.
This is just one of many reasons. But it's a big one. Hospital-employed anesthesia just doesn't have the flexibility for cost savings like bigger groups do.
All this "data" these companies collect regarding "compensation" is worthless unless hours worked/acuity of cases are taking into context.
I have the 2015 MGMA data for anesthesia (sorry can't share it publicly since it was purchased...anyone can buy it) but it only breaks by ownership/amc/hospital (but not actual hours worked or acuity of cases (asa 1-4) and average vacation time (roughly 8 weeks).
Me personally
You are forgetting out of OR needs (GI/EP etc) plus OB coverage (even at light OB hospitals it's still coverage needed)
The GI guys do all their lucrative private insurance at their outpatient GI center than decide to show up between 11am-2pm expecting "coverage" for their sicker Medicare/Medicaid inpatients (or outpatients done in the hospital).
Also some busy ortho practices basically demand 2 rooms as well.
So 10 ORs daily really means (assuming 80%-90% capacity daily from 7-3pm) plus out of OR plus certain surgeons demanding 2 rooms (say they have 6 shoulders).
You are gonna to need 12 bodies (3 MDs covering 12 crnas or 12 MDs if all MD model). And that's running things tight for "10 ORs plus GI/EP/OB"

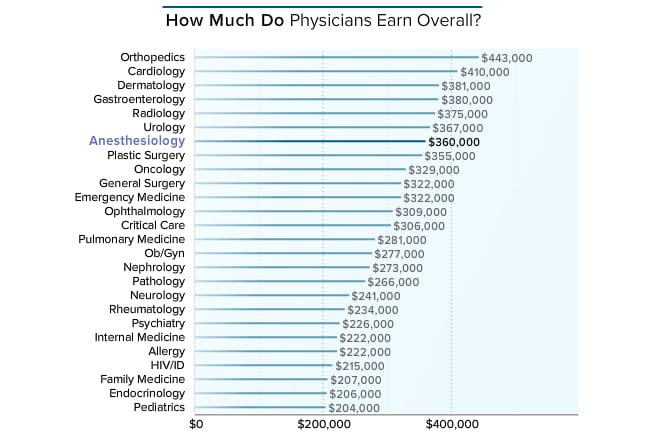
Medscape Anesthesiologist Compensation Report 2016
Carol Peckham | April 1, 2016
Anesthesiologists who responded to this year's Medscape compensation survey disclosed not only their compensation but also how many hours they work per week, how many minutes they spend with each patient, the most rewarding part of their job, changes to their practice resulting from healthcare reform, and more. (Note: Values in charts have been rounded and may not match the sums described in the captions.)
Physicians were asked to provide their annual compensation for patient care. For employed physicians, patient-care compensation includes salary, bonus, and profit-sharing contributions. For partners, this includes earnings after taxes and deductible business expenses but before income tax. When asked about their compensation for patient care, anesthesiologists were seventh from the top ($360,000), slightly lower than in last year's compensation report ($358,000), when they were fourth from the top. Orthopedists and cardiologists were numbers one and two this year ($443,000 and $410,000, respectively) and last year as well, at $421,000 and $376,000. Within these specialties there is likely to be a wide range of earnings, as orthopedics and cardiology both include surgical subspecialists, who tend to make significantly more than their generalist counterparts.[1]
Anesthesiologists had a 1% increase in income this year, near the smallest among all physicians.
Anesthesia salary has been very stagnant in the last 5 years or so...not surprising.
My guess is a mere $2,000 is within the margin of error of the sample size. Bottom line is that no one can honestly say anesthesiology with tangible evidence that salaries are currently in decline over a prolonged time period. It would be a completely ridiculous statement.
My guess is a mere $2,000 is within the margin of error of the sample size. Bottom line is that no one can honestly say anesthesiology with tangible evidence that salaries are currently in decline over a prolonged time period. It would be a completely ridiculous statement.
Anyone without connections in this job market knows that salaries are in decline and the number of good jobs available are sparse. I have already argued this point with you and see no reason to continue the debate. I'll just say we disagree on this issue. As in most professions there are great jobs out there paying a lot of money with decent lifestyles. The problem is the number of those jobs keeps getting smaller and smaller each year driving wages to the $360K median with longer hours at work.
In 2009 it wasn't that difficult to land a $450K gig even using gaswork.com. In 2016 the number of jobs advertising that salary is just a few and most of them are quickly taken by Anesthesiologists without connections. Again, I contend real salaries are down 25% in 2016 vs 2009 and if you don't have any connections to the fewer good gigs out there be happy earning anything over $425K.
I think the average salary figure would be more indicative of whether salary has indeed being going down based on the theory that there are less and less private practice gigs that pay over 450k per year...im interested to see whether or not blademada assertion is true that salaries have been pushed closer to the median of 360k.
The problem is you still have nothing but flippantly stating anecdotal stories. Nothing. Zilch. Nada. You have literally no evidence to back up your claim that anesthesiologists are making less money. Mednax skimming off the top needs context in the face of their higher demanded revenue units. Gaswork.com is about as scientific as me just saying I talked to Joe Bob in the doctor's lounge the other day.
You are doubling down on an asinine prediction you made. That's all this is. For the folks reading at home. Just admit you were wrong and move on. Sheesh.
By 2015 the DNAP CRNA should be in place for some schools. I suspect the Obama Health Care plan will be in full swing as well.
My conjecture is that MD Anesthesiology income is reduced 25-30% from today's levels. CRNA income should hold at today's levels but I am not sure if cost of living is keeping up with the dollar now known as hard toilet paper.
Anyone else care to speculate?
I should have clarified my original post to state "Private practice MD Anesthesiology income would be reduced by 25%." I do admit that perhaps my timing was off by 1-2 years but I stand by the original post.
Maybe. If you are an employee drone, then your income will be down for sure. I'm not convinced about private practice although you will probably be working harder.
Agree.The trend is very clear that there will be many more drones working for "the man" next year.
There is no PP anymore, in many areas. There is just PP employment, for most new grads. Which is not much different than any other employment, including AMC.Maybe. If you are an employee drone, then your income will be down for sure. I'm not convinced about private practice although you will probably be working harder.
There is no PP anymore, in many areas. There is just PP employment, for most new grads. Which is not much different than any other employment, including AMC.
True PP is still out there despite the fear and loathing that is often propagated around here.

160 groups will have sold out to Anesthesia management companies since 2009. 160 groups is NOT nothing. What was the salary in these groups when you include bonuses? $550K for the median? What is the salary now for that same job when a new graduate applies? $350k? Yet, you continue to post the most asinine statements that things haven't changed in this field when in fact there is a paradigm shift to EMPLOYMENT at the median wage level (which was never correct in 2009 to begin with). In addition, dozens of other groups have been terminated by hospitals across the country and forced to become employees. The wages of these Physicians are now much lower.
I won't admit to someone without an understanding of basic economics that salaries haven't gone done based on a survey of 4-6% of Anesthesiologists many of whom are in academics or other lower paying positions. The fact is the Median wage for private practice Anesthesiologists is down due to the surge by AMCs and hospitals in taking over anesthesia groups. Many new graduates and certainly future CA-3s are looking at a much more difficult job market with less opportunities than those who finished residency in 2009.
Yet 7 years ago you attributed this to Obamacare and cRNA encroachment. Now, you've built a strawman trying to save your cred by sounding prophetic. And even still, you were waaaaay off in your prediction and have zero published numbers to back it up.
Yet 7 years ago you attributed this to Obamacare and cRNA encroachment. Now, you've built a strawman trying to save your cred by sounding prophetic. And even still, you were waaaaay off in your prediction and have zero published numbers to back it up.
Actually, CRNA encroachment has contributed to erosion of compensation (let's not use the word salary, since you are correct in pointing out that salary has not changed on the surveys). The flooding of the market with CRNAs from these SRNA schools that open up all over has contributed to a decline in our value in the eyes of many administrators. It's simple supply and demand. Again, this decline in compensation and value that we are seeing is multifactorial. You can't point your finger at one particular cause.
Sitting back and saying compensation has not only stayed the same, but has improved is both wrong and irresponsible. It's this kind of passivity among doctors as a whole that has gotten us into this situation in the first place. The decline in physician compensation (increased workload, decreased reimbursement) is only one small symptom of the problems in this current healthcare system. It is those among us who show discontent with the status quo that become the rabble rousers we need to affect change. If our patriot forefathers were content paying all those taxes levied by the British (even though many of them could afford it), we would not have a reason to have barbecues and fireworks this weekend.
I'm not sure why so many groups have sold out. Was it Obamacare? Was it all the regulations found inside the ACA? is it because hospitals are slashing stipends? I concede that the exact cause for this large sell-out was not due to CRNA encroachment. As for my sounding "prophetic" I"ll let those who read this entire thread decide for themselves whether the fact that 4,000 Anesthesiologists have moved from private practice to "employee" since 2009 is indeed a big paradigm shift with a significant effect on salaries. Again, I see your viewpoint on salaries but vehemently disagree with it and firmly believe that "average" new resident seeking private employment today will likely earn significantly less money overall in private practice than in 2009 due to this huge paradigm shift.
Those who are just entering this field as Residents or considering it as Med students need to see all of the facts, both good and bad, to make an informed decision about their futures. The evolution of Anesthesiology from private practice to employee has accelerated rapidly since 2009 and the search for true private practice is now much harder than in the past.
BS. I have actual statistical data. You have nothing. The only thing dangerous is posting made-up, egotistical drivel on a public message board that could drive away good minds from the future of the specialty.
Again- you are trying to sound right by saying there has been a shift in the way anesthesiologists business is set-up. Guess what? In 7 more years we will likely say the same. One constant in this world- change.
No, to those reading, no medical specialty will be the same 7 years from now.
So do what you like to do and you can't go wrong.
I was talking to a urologist I work with. Medicare is going to start reimbursing a robotic prostatectomy to $800 from $1200. An ENT told me myringotomies/ear tubes are having their CMS reimbursement rates slashed as well. Radiology reimbursement has been hurting for years now.
It's all across medicine. Politics are alive and well in medicine. And as a result, we may all hurt.
BS. I have actual statistical data. You have nothing. The only thing dangerous is posting made-up, egotistical drivel on a public message board that could drive away good minds from the future of the specialty.
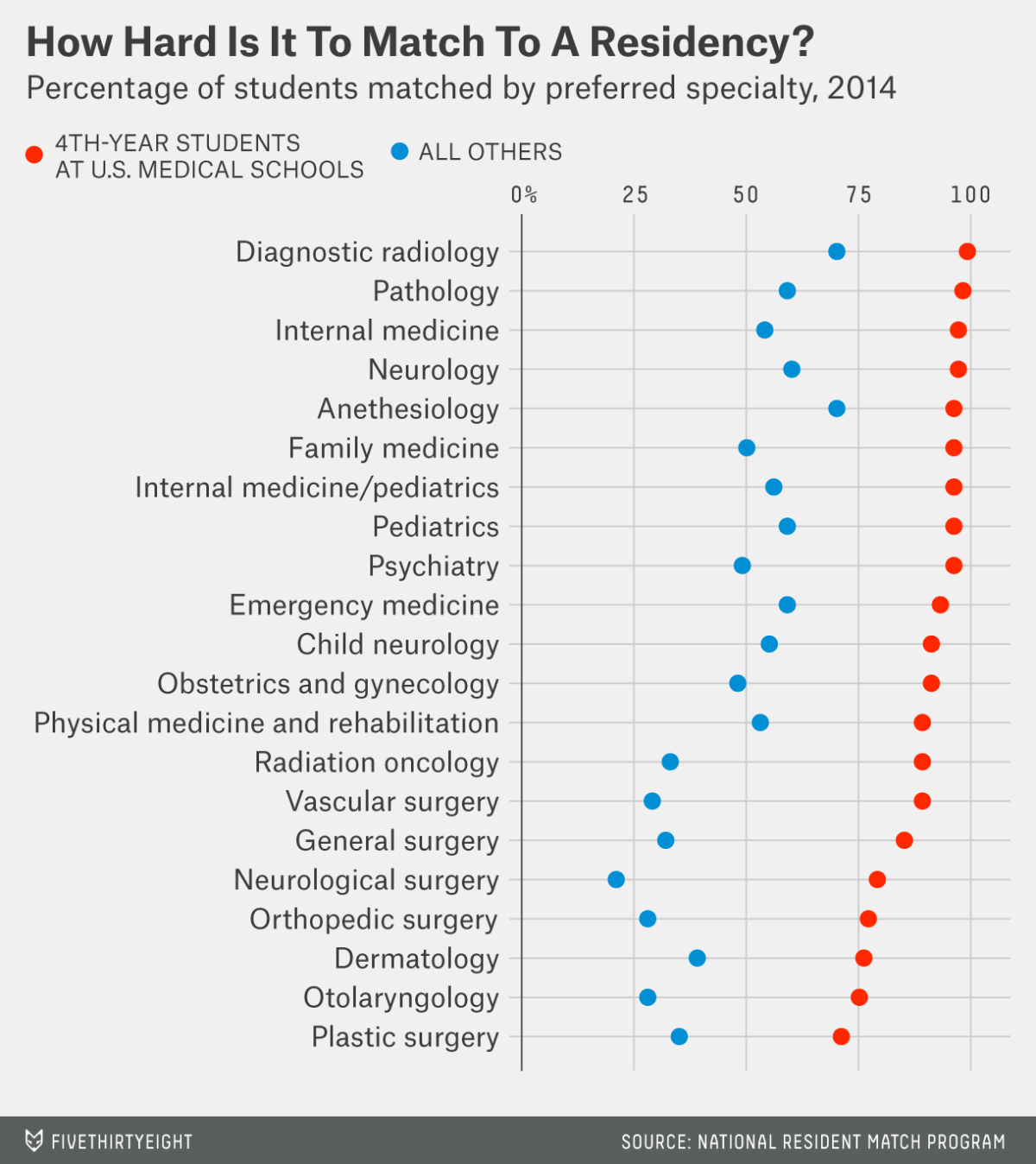
This graph is useless since it doesnt factor in self selection...
Helpful, though I wish they had made distinctions in the "All Others" category (e.g., DO, US-IMG, IMG).
I think it does factor in self selection. How many Med Students are gunning for Derm with Step score of 210 vs Family Practice or Anesthesiology?
A high Step 1 score and you get to pick your specialty. A low Step score and the bottom rung is what you get stuck with.
Great pie chart.
By your logic blade the total amount paid into the practice anesthesia has gone way up since 2009. With all the AMC buyouts insurance companies and hospitals are paying more than ever for anesthesia services...the only problem is that most of the money is know going to Wall Street and the venture capitalist backing the buyouts.
Again know your worth.
Correct. The per Unit charge for anesthesia is up 30-50% since 2009. This means private practice income should be in excess of $450-$500K (plus the benefit package). The fact that someone on here thinks $360 or even $400K represents an "increase" in compensation since 2009 is truly ignorant. This is why I stress one should seek out true private practice rather than an "employee" position. As of 2016 there are still opportunities out there in the private sector.