About the "disconnect"...
Some of us who are more established in our jobs and have it good remember when we had/could've had it even better. I entered med school 15 years ago and ensconced myself in rad onc world 14 years ago. It is not exaggeration to say that rad onc was a bubble at that time. I fully expected to be making 750k-1mil mid career with an ownership stake in my own linac/clinic, full autonomy to practice how I saw fit, command respect at tumor boards, and participate in important clinical research. All of that had crash landed 7 years later by the time I started practice, and I got a much watered down version of my expectation. Perhaps the expectations were too lofty, but they were the reality at the time. Still love my life and my job. I work a bit harder for less money, ownership, respect, etc... but it's still really good.
Guys coming out today weren't really around for this bubble time and see making 350k for an easy gig, in an adequate place, while being a cog in the system of a teetering field for some chairman/CEO as being perfectly acceptable. And it still is. 7 years later, they are essentially getting a further watered down version of what I got. Still a good job that 99.9999% of the world would love to have etc, etc... Hell, I'd probably do it again if I was guaranteed this outcome.
But.... The same trends that drove the changes I've seen during the past 2 two seven year intervals (declining reimbursement, declining autonomy/increased scrutiny, no ownership potential, intellectually bankrupt academia) all continue and worsen by the year, but now with the added threat of supply/demand imbalance and payment model. Current medical students are probably on a seven year horizon. I am definitely not bullish on the future job prospects at that time interval having witnessed the change that has occurred during the last two.
I would hazard to say those trolling every post here with the only the rosiest colored glasses may have some ulterior motive. They may not even be entirely (read: at all) truthful about their position in all this mess.
For my part, it always comes back to math. Less money (whether due to less fractions/indications/utilization or APM or whatever) + More Rad Oncs to fight for that money = The future for rad onc. You can argue however you want, but there is no denying math.
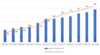
But, but, but... there are more old people now than 20 years ago. Really? Are there more that twice as many old people? Because there are twice as many rad onc residents per year and average reimbursement per patient has dropped for years.
But, but. but... oligomets are a thing now. True. Not that they weren't before, but we treat more of them than we used to. Pending payment reform (bundling), I can't see "bone met" or "lung met" or "brain met" being particularly highly compensated indications for radiation but maybe I'm wrong. Certainly not enough to make up for losses elsewhere.
This continues to be the issue. Trends are unfavorable, math is unfavorable, future is ___________? No one knows for sure, anything can happen in 7 years, but buyer beware.