- Joined
- Apr 16, 2004
- Messages
- 4,658
- Reaction score
- 5,069
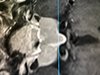
I'm seeing a patient in her early 50s who presented with severe migraine HAs and did not respond to conservative medical management. Her PCP eventually ordered an MRI Brain which revealed a pituitary macroadenoma which extended into the R cavernous sinus.
She underwent visual and endocrinology testing, both were negative. She underwent a trans-sphenoidal resection and the sellar and suprasellar components were removed. Headaches resolved post-operatively.
We are now wondering what to do with the ~ 2 cm remnant in the R cavernous sinus. It has remained unchanged 8 months post-op. I was going to offer her adjuvant XRT, but one of my colleagues suggested bromocriptine, despite this adenoma being non-functioning.
Have you every heard of this?
She underwent visual and endocrinology testing, both were negative. She underwent a trans-sphenoidal resection and the sellar and suprasellar components were removed. Headaches resolved post-operatively.
We are now wondering what to do with the ~ 2 cm remnant in the R cavernous sinus. It has remained unchanged 8 months post-op. I was going to offer her adjuvant XRT, but one of my colleagues suggested bromocriptine, despite this adenoma being non-functioning.
Have you every heard of this?