
- Joined
- Feb 10, 2006
- Messages
- 22
- Reaction score
- 0
About 2 weeks ago, I was exercising and applied pressure to something in my left brachial plexus just proximal to my shoulder. During and after this incident, I experienced sensory and motor disruption initiating along my left arm, beginning at my left thumb and spreading up throughout the forearm all the way up to and including my shoulder.
In the 2 weeks since, I've had paraesthesia affecting all of the left arm. This remains most significant at the base of my thumb. Some sensation seems to have returned. However, in addition, I currently have, at most, half the strength in my left arm/hand/wrist compared to my right. X-rays have shown no non-neural injury.
I just came back from a physiatrist for a nerve conduction study. He took a quick glance and stated exclusively that the results were 'within normal range'. However, it was less than a thorough examination, and at one point, he even told me that "lat (m/s)" on the printout stood for "lateral", not "latency".
Furthermore, this situation is somewhat disheartening to me, as, in addition to med student, I'm an avid drummer/guitarist, and the full strength and dexterity of my hands/wrists is quite necessary for both. Currently, I am functioning at a significantly reduced capacity, and it's been pretty difficult to handle as a result.
Based on that, I still have questions about the nature of the injury and prognosis, and I was hoping one of the fellow students a little farther along than me in their education might be able to lend some assistance.
Testing was done in my wrists and fingers. Again, it is the left side that was injured.
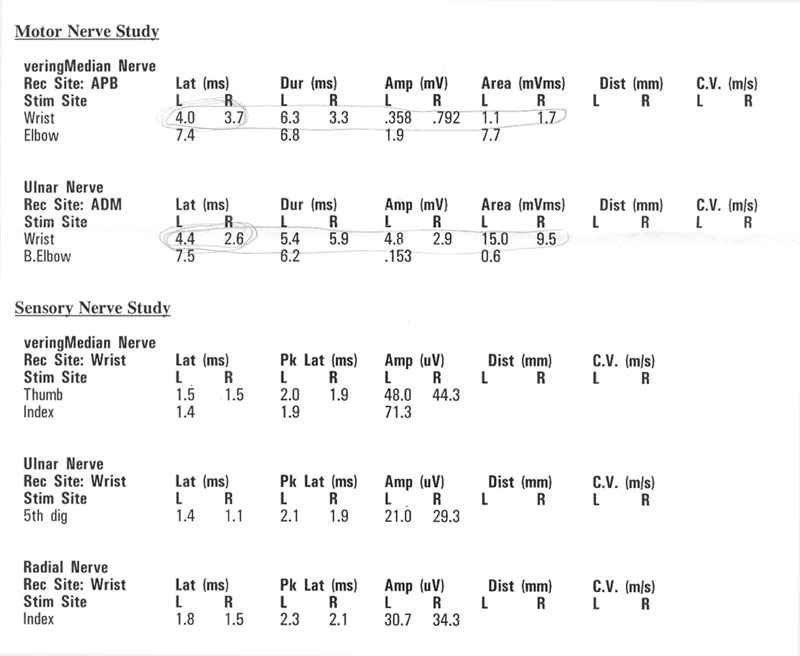
My Observations:
- Latency is higher in left limb by 8%, 69%, 0%, 27%, and 20%.
- Left median motor amplitude is 45% of right; left area is 41% of right.
- Left ulnar motor amplitude is 66% higher than right; left area is 58% higher than right (?).
Any help interpreting the data above a bit more thoroughly would be greatly appreciated.
Im still hoping its purely simple neuropraxia with a couple more week recovery window. However, the latency and amplitude differences, as well as minimal improvement thus far, make me wonder if it might be more severe with a much longer (and possibly incomplete) recovery, like, additionally, a partial axonotmesis.
Thanks in advance,
Mike
In the 2 weeks since, I've had paraesthesia affecting all of the left arm. This remains most significant at the base of my thumb. Some sensation seems to have returned. However, in addition, I currently have, at most, half the strength in my left arm/hand/wrist compared to my right. X-rays have shown no non-neural injury.
I just came back from a physiatrist for a nerve conduction study. He took a quick glance and stated exclusively that the results were 'within normal range'. However, it was less than a thorough examination, and at one point, he even told me that "lat (m/s)" on the printout stood for "lateral", not "latency".
Furthermore, this situation is somewhat disheartening to me, as, in addition to med student, I'm an avid drummer/guitarist, and the full strength and dexterity of my hands/wrists is quite necessary for both. Currently, I am functioning at a significantly reduced capacity, and it's been pretty difficult to handle as a result.
Based on that, I still have questions about the nature of the injury and prognosis, and I was hoping one of the fellow students a little farther along than me in their education might be able to lend some assistance.
Testing was done in my wrists and fingers. Again, it is the left side that was injured.
My Observations:
- Latency is higher in left limb by 8%, 69%, 0%, 27%, and 20%.
- Left median motor amplitude is 45% of right; left area is 41% of right.
- Left ulnar motor amplitude is 66% higher than right; left area is 58% higher than right (?).
Any help interpreting the data above a bit more thoroughly would be greatly appreciated.
Im still hoping its purely simple neuropraxia with a couple more week recovery window. However, the latency and amplitude differences, as well as minimal improvement thus far, make me wonder if it might be more severe with a much longer (and possibly incomplete) recovery, like, additionally, a partial axonotmesis.
Thanks in advance,
Mike