- Joined
- Nov 21, 1998
- Messages
- 12,547
- Reaction score
- 6,932

Agree this is insane far left liberal nonsense.
People have to take personal responsibility, the state shouldn't do everything for them.
the otherspeak to what you are pontificating about is that safe injection practices and supervised injections would reduce the risk of endocarditis, reduce the risk of futile end of life ICU care (due to accidental OD), reduce the costs of Hep C amongst those who are still negative, and decrease overall costs of healthcare bills to the community. reduce the power of cartels, and decrease the "need" to get involved in prostitution, trafficking and torture because they will have a safer place to shoot up.
I don't agree with this, mind you. I think it is condoning the practice of illicit drugs
but they are actually using your "arguments" as grounds for setting up these safe injection sites - supervised injection sites may decrease certain societal burdens...
the otherspeak to what you are pontificating about is that safe injection practices and supervised injections would reduce the risk of endocarditis, reduce the risk of futile end of life ICU care (due to accidental OD), reduce the costs of Hep C amongst those who are still negative, and decrease overall costs of healthcare bills to the community. reduce the power of cartels, and decrease the "need" to get involved in prostitution, trafficking and torture because they will have a safer place to shoot up.
I don't agree with this, mind you. I think it is condoning the practice of illicit drugs
but they are actually using your "arguments" as grounds for setting up these safe injection sites - supervised injection sites may decrease certain societal burdens...
Agree this is insane far left liberal nonsense.
People have to take personal responsibility, the state shouldn't do everything for them.
how do you know they want to die? i thought they wanted to get high... im sure their family members don't want them to die.
and id hate to see what other populations can be "eliminated" if we argue burden on society.
As has already been stated, it is the libertarian faction that supports this BS. Don't drag liberals into this
Even more interesting is that lyrica and several other scheduled drugs are tested on these patients in Canada . Maybe some of the Canadian physicians can enlighten us on this governmental opioid project . Does it have any societal benefits that has been provenIt will be interesting to see Vancouver's data tracking the rate of overdose deaths and detox utilization
http://www.theglobeandmail.com/news...re-overdose-prevention-sites/article33276659/
http://www.theglobeandmail.com/opin...ives-and-must-not-be-illegal/article33329479/
I disagree. Liberals want the government to take care of every single potential problem in life, no matter what the cost in taxes, and irrespective of whether or not the government is actually good at solving the problem.
there are a few libertarian socialists in Europe, however in America libertarians want minimal government and would rather that the individual be responsible for his/her successes and failures in life.
This proposed coddling of addicts, by the state paying for rooms for addicts to shoot up in hospitals is in direct opposition to the libertarian position of the majority of American Libertarians, and is much more in line with position of American liberals and the Democratic Party.
A little off topic but I thought I would also make this known.
I have gone from a previous private practice to now hospital employed.
I see patients in a free standing outpatient clinic.
I was asked by the hospital admin about potentially seeing patients in a clinic on the second floor of the hospital.
I recently found out, that when other physicians see patients on hospital campus and not in the outpatient medical office building, hospital is charging a facility fee in addition to my usual 99xxx clinic codes.
They have apparently been doing this for several years to a couple of decades.
i understand you do not want physicians to shoulder any of the "blame" with regards to the opioid situation. think of it this way - Big Pharma and the desire to make $$$ lead to this problem. and I understand you don't want to affect potential livelihood in pain in any way.Correct.
Liberals also would like to blame doctors or some other force besides the JUNKIE themselves for the problem.
Ergo, even when prescription opioids decrease by 30%-40% with ZERO difference in overdose rates due to junkies going on the streets to get heroin/coke/etc, these liberals will continue to strawman the issue to blame someone else besides the junkie.
The next liberal argument will be the "doctors caused the junkies to get these drugs off the street, therefore, its their fault!". Just wait a few years and that will be the new mantra after rates of overdose don't decrease.
Reminds me of the Chicago murder rate situation with the police. If the police go into bad areas to crackdown hard, they are "racists" who are treating people like "animals" and therefore are causing hoodrats to murder each other because they are "dehumanizing them".
Yet when the police pull out and the murder rate goes UP, the police are GUILTY again for abandonment of the "vulnerable" populations.
Damned either way.
i understand you do not want physicians to shoulder any of the "blame" with regards to the opioid situation. think of it this way - Big Pharma and the desire to make $$$ lead to this problem. and I understand you don't want to affect potential livelihood in pain in any way.
but 2 points -
1. you use the argument that we should not do any procedural interventions due to the dearth of EBM. well, it is even worse for COT.
2. the problem with your argument is that the drugs already caused the junkies to exist. even if physicians do decrease opioid prescribing, I agree it will probably not affect the rate of the # of junkies OD'ing. they are a lost generation - Legacy patients. it may even be too late for their children, who see and become exposed via their parents.
opioid reduction is for the future, for the next generation to avoid the exposure.
And here it starts, and I think it's near Ligament: http://www.seattletimes.com/seattle...n-sites-get-ok-from-king-county-health-board/
Lets make it safer and more convenient so we can foster an even larger junkie population. The liberal mindset is an offense to logic.
Have any of you guys been to Vancouver, BC? It is flush with junkies and ever expanding. What a great objective to have as a city.
i understand you do not want physicians to shoulder any of the "blame" with regards to the opioid situation. think of it this way - Big Pharma and the desire to make $$$ lead to this problem. and I understand you don't want to affect potential livelihood in pain in any way.
but 2 points -
1. you use the argument that we should not do any procedural interventions due to the dearth of EBM. well, it is even worse for COT.
2. the problem with your argument is that the drugs already caused the junkies to exist. even if physicians do decrease opioid prescribing, I agree it will probably not affect the rate of the # of junkies OD'ing. they are a lost generation - Legacy patients. it may even be too late for their children, who see and become exposed via their parents.
opioid reduction is for the future, for the next generation to avoid the exposure.
Clearly, in areas where opioid prescriptions have gone down the most, there has been no morality decrease. These people just get on other drugs.
and aren't you the one who rails against cardiac caths, fusions, C-sections, etc.? or is there another drcommonsense?
is there level 1 evidence for ESI? even RFA has some equivocal level evidence...
no, you miss the point entirely. the opioid epidemic primed the pump. reducing the opioid prescribing rate will not touch the overdose rate, not til the at risk portion of this generation is gone - either dead, or rehabbed.
as an example, we are making progress in reducing the rate of smoking. that rate is going down much faster than the rate of developing cancer, but smoking related cancer is still high.
no offense taken...just that van had a much larger (yet somehow better isolated) junkie population until recently, until Seattle thought it would be a good idea to attract junkies by offering free campgrounds and housing and food. Now Seattle has homeless encampments spread throughout the city, and it is growing. How about we attract working folk with skills only, as opposed to homeless? WTH?No offense lig, but I found Vancouver to be a sister city to Seattle in most ways. Both cities are extremely liberal, and hippie central.
oh that's an easy one commonsense. and the article notes it too. its about availability.
first, you can clearly see that there is an upward trend of opioid painkiller OD and a downward trend in heroin OD. that in itself should be easy to understand. take whats available, and "safer" or "cheaper" or "doctors orders"...
in 2010, Purdue reformulated oxycontin so it was more difficult to crush and more tamper resistant. it took about 4-5 months before someone figured out how to break through. even then, apparently not worth the effort, according to SWIM on opioiphile.org forums.
your article states: "people who were pill users in 2013 were much more likely to be heroin users in 2106, but were no longer pill users. In other words, drug abusers switched from pills to injectable narcotics during a time when the pills were becoming more difficult to obtain."
and yes, that suggests that opioid restricting will not affect these victims.
but my point all along is that a main reason to decrease prescribing is so that fewer people will start using pills - and subsequently get addicted - in the first place. those who have started are already a lost generation.
that's why a snapshot of heroin OD rates will not significantly change, until the current patients that got addicted to prescription opioids die or learn to manage their addiction.
I hate to say this, but you don't seem to remember when opioid prescribing was not the norm.
The current generation got addicted because they were given opioids or stole them from people who were given them.
There is no debating the fact that the majority of patients now using heroin started with non heroin opioids.
I agree the majority of these people will never get better.
As I stated before, a primary reason to decrease prescribing is so the the next generation doesn't get addicted too. There's still hope for the kids...
Sent from my iPhone using SDN mobile
omg. where have you been hiding these past 15 years?
and making multiple assumptions about what I want.
who is at fault is Big Pharma and the desire of some doctors to put profit over patient care.
before I post probably 30 some odd articles clearly linking the current opioid epidemic and heroin use increase, let me be point blank in that your "liberal" solution is not anywhere close to what would be "my" solution.
first, you define what are "legitimate narcotics".
I will discuss "appropriate opioid" medications. "Narcotics" are a legal term. we (at least I) am a physician. (your elderly patient needs to know how to safely store his/her opioid medications with a lock box and be told that under no circumstance
second, addicts should have access to addiction treatment. this may include a short course of suboxone.
third, there are bad seeds that are doctors. the DEA and state DOH is responsible for finding out who they are. most doctors are not bad seeds, but some get duped by money grubbing pharmaceutical companies advertising false lies all for more and more money.
I agree. Docs have been complicit but, unless you are a pediatrician, I don't think you "make" an addict out of an emotionally healthy individual. Except maybe the very rare case.I never said there weren't "bad docs", I am just strongly unconvinced there is a large segment of non-mentally ill/depressed/addict personality patients that are getting addicted to opioids randomly.
I agree. Docs have been complicit but, unless you are a pediatrician, I don't think you "make" an addict out of an emotionally healthy individual. Except maybe the very rare case.
over 100,000 people dead from prescription opioid overdoses.Managing chronic nonmalignant pain: overcoming obstacles to the use of opioids.
Passik SD1, Weinreb HJ.
Author information
Abstract
- 1Oncology Symptom Control Research, Community Cancer Care, Inc., Indianapolis, IN 46202, USA.
Physicians involved in cancer pain management treat thousands of patients with opioids, whose effective analgesia improves overall functioning. Side effects generally are tolerable, and treatment can be maintained with stable doses for long periods. Problems with addiction are infrequent. Many physicians, however, assume that opioids should be used only for chronic malignant pain. Research and clinical experience have demonstrated that opioids can safely and effectively relieve most chronic moderate to severe nonmalignant pain. Fears of addiction, disciplinary action, and adverse effects result in ineffective pain management. With current information on the use of opioids in chronic nonmalignant pain, primary care physicians can overcome these obstacles. Guidelines must clearly define the role of the primary care physician in the proper management of pain and the integration of opioid therapy. Used appropriately, opioids may represent the only source of relief for many patients.
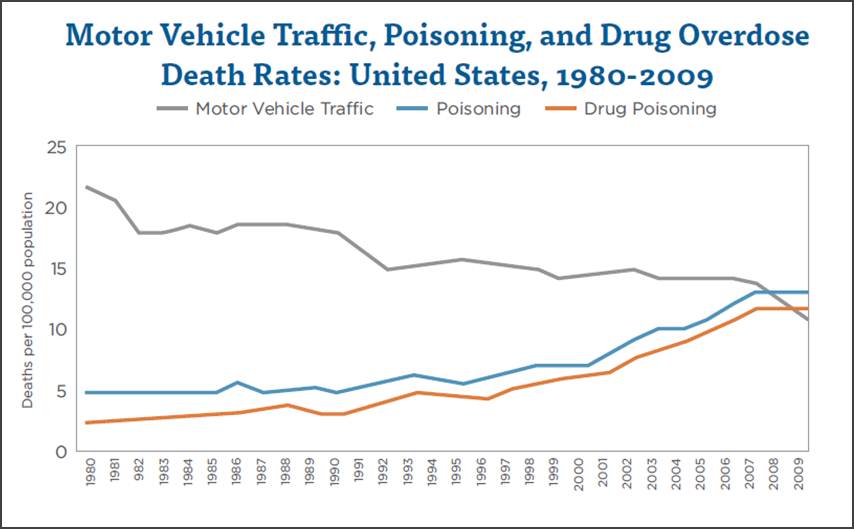


heroin abuse rates, when you look historically, are relatively unchanged from 1980s to present. 500,00 - 600,000 Americans.
what is different:
the rate of prescription opioid abuse and death.
take home message - the druggies have always been out there. making changes towards appropriate opioid prescribing will not affect them, I agree.
but everyone else...
heroin abuse rates, when you look historically, are relatively unchanged from 1980s to present. 500,00 - 600,000 Americans.
what is different:
the rate of prescription opioid abuse and death.
take home message - the druggies have always been out there. making changes towards appropriate opioid prescribing will not affect them, I agree.
but everyone else...
the problem is that you are relying on an article that is in itself is primarily focused on recommending increased substance abuse treatment - ie more suboxone, which a few here have derided as a money making scam.
for example, the article states "In addition, looked at from the chronic pain treatment perspective, studies find that very low percentages of people who do not have previous drug abuse histories become addicted during pain care."
if you review the link, however, you find this: "Signs of opioid addiction were reported in 0.27% of participants in the studies that reported that outcome. All three modes of administration were associated with clinically significant reductions in pain, but the amount of pain relief varied among studies. Findings regarding quality of life and functional status were inconclusive due to an insufficient quantity of evidence for oral administration studies and inconclusive statistical findings for transdermal and intrathecal administration studies."
and you did not post the take home message on that article, which i agree with wholeheartedly:
"Up to 8 million chronic pain patients are estimated to currently receive opioid prescriptions; the vast majority of them do not have addiction problems. Certainly better oversight to ensure appropriate prescribing is needed to prevent future addictions and to target opioid treatment to those who will benefit. But today, simply reducing the legal supply will only increase the illegal market.
In order to really address the opioid problem, we need to rapidly expand evidence-based maintenance treatment – and figure out why so many Americans are turning to the most dangerous drugs to self-medicate."
(bold emphasis is mine)
im sorry you fail to see the logic in limiting supply so that addicts cannot steal their fix from family and friends, if the family/friends do not have opioid medication lying around.
https://www.drugabuse.gov/publicati...vailability-associated-increased-use-overdose