- Joined
- Feb 1, 2005
- Messages
- 4,899
- Reaction score
- 1,882
View attachment 292129
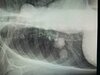
Young guy. Axial extension-based pain with bilateral L5 pseudoarticulations that I suspect are the primary pain generator. I want to inject for diagnostic and therapeutic reasons but unsure where exactly I should target my needle -- thinking the inferolateral corner of each L5 transverse process. Any thoughts?
When in doubt exam under fluoro to confirm precise tender area facet vs pseudoartic vs si.