- Joined
- Dec 18, 2015
- Messages
- 3,216
- Reaction score
- 4,930

Rather striking...
Ralph and David Kirsch probably kept calling and texting the editors with "plz don't publish this, it expands the indications for XRT"Rather striking...
View attachment 329026
It took them 5 months to accept it? This is a 2 case report!!!
That there's an even 1% chance your theory is true is quite sad... because were it true, this treatment would have the highest reward/risk ratio of any radiotherapeutic treatment ever devised or theorized in the history of mankindI will go on believing that we could have saved literally dozens of thousands of lives in America and likely hundreds of thousands worldwide had we been a bit more forward thinking and aggressive in optimizing low dose XRT early in the pandemic.
Huge failure for our specialty.
EDIT: I understand this belief isn't rooted in overwhelming evidence.
Yeah but that's like, what, a tenth of a centigray a day versus 0.1 cGy per weekSomeone should do a retrospective review and see if the intubated patients who got the obligatory daily bedside CXR to ensure proper ET tube placement did better than those who only got weekly films.
"Obviously, either intervention yields a 30% treatment induced death rate at 5-years."Yeah but that's like, what, a tenth of a centigray a day versus 0.1 cGy per week
All radiation matters!Yeah but that's like, what, a tenth of a centigray a day versus 0.1 cGy per week
Maybe a close second to vaccination, but yes.That there's an even 1% chance your theory is true is quite sad... because were it true, this treatment would have the highest reward/risk ratio of any radiotherapeutic treatment ever devised or theorized in the history of mankind
I am not a big fan of dragging but Ralph and David should be dragged so so hard for such a silly, wasteful, yelling-fire-in-a-crowded-theater response to this. It hurt my heart!"Obviously, either intervention yields a 30% death rate at 5-years."
-Ralph Weichselbaum, probably
I will go on believing that we could have saved literally dozens of thousands of lives in America and likely hundreds of thousands worldwide had we been a bit more forward thinking and aggressive in optimizing low dose XRT early in the pandemic.
Huge failure for our specialty.
EDIT: I understand this belief isn't rooted in overwhelming evidence.
Rather striking...
View attachment 329026
It took them 5 months to accept it? This is a 2 case report!!!
Maybe fractionation plays a role?Someone should do a retrospective review and see if the intubated patients who got the obligatory daily bedside CXR to ensure proper ET tube placement did better than those who only got weekly films.
It's ULTRA!sigh.... 2 cases.....
The funny (sad) part is that the inherent bias against radiation was so strong amongst those that get paid to deliver radiation.
We are truly a self loathing specialty.
Man, I don't know if this is a precedent we want to set, potential court battles coming in 3...2...1...Here's an update from Emory.

Response to Whole-Lung Low-Dose Radiation Therapy (LD-RT) Predicts Freedom from Intubation in Patients Receiving Dexamethasone and/or Remdesevir for COVID-19-Related Acute Respiratory Distress Syndrome (ARDS)
Background Phase I/II clinical trials have explored whole-lung low-dose radiotherapy (LD-RT) as a potential treatment for patients with COVID-19-related acute respiratory distress syndrome (ARDS). Initial findings require reproduction. Concomitant LD-RT administration with existing therapies...www.medrxiv.org
20 patients matched to 20 controls. It's a pre-print.
Astonishingly is however this:
View attachment 331405
Excuse me, but how does that exactly "work"?
Provided, LD-RT is shown to be the "game changer" in a randomized trial in the future and becomes standard of care, will we have to pay Dr. Hess and Dr. Khan in order to deliver it?
"LD-RT technogy" surely sounds complicated, no wonder it's patented...
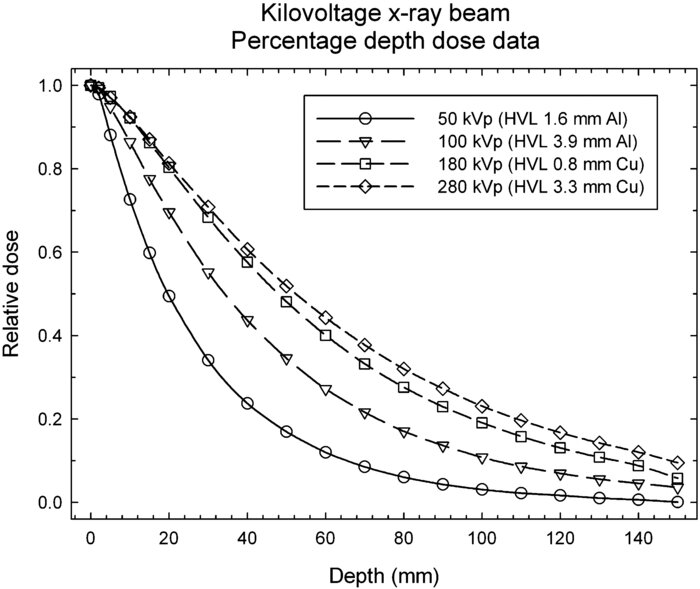
"A single treatment of 1.5 Gy to the bilateral whole lungs with 15 megavoltage photons on a linear accelerator, utilizing a 2-dimensional therapeutic radiation technique, an anterior-posterior beam configuration, and standard dose rates (600 MU/min)."
I've never seen that before...
My bet is some orthovoltage X-ray machine on wheels...Found (marginally) more info from this site:
View attachment 331416
So it seems like it's equipment, not the technique itself, which makes WAY more sense.
Indeed.My bet is some orthovoltage X-ray machine on wheels...
Indeed.
However it will not be trivial to deliver the 1.5 Gy WLI with an orthovoltage machine resulting in a homogeneous dose distribution in the lung. Even you go for 200-300kV with a.p./p.a.-fields, you still have something like 25+ cm of lung to irradiate through. Dose distribution will not be nice.
Oh lordy. That'd be over-over-engineered for ~1 Gy to the lungs. (But I wouldn't put it past Mo Khan lol.) Just use something like this right here...Maybe it's like an iron lung that uses MV beams... like a SBRT version of Zap-X?

@LoudChicken,
Do you work at Emory and have data?
I am just curious who to believe, the authors on medrvix.org or an anonymous whistle-blower?
"No other toxicity, airway emergencies, or adverse events were observed." You know, other than the 20% mortality. To get around this, they classify those who ended up dying as "non-responders", and compare all the controls against the "responders." The study is an absolute joke.
You'd never know from the tweet that 20% of the radiation treated group died, compared to 0% of controls.
What would the skin dose be if tried to deliver 1 gy whole lung with ortho voltage?Indeed.
However it will not be trivial to deliver the 1.5 Gy WLI with an orthovoltage machine resulting in a homogeneous dose distribution in the lung. Even you go for 200-300kV with a.p./p.a.-fields, you still have something like 25+ cm of lung to irradiate through. Dose distribution will not be nice.
Assuming ~300 kV and 0.5 Gy from the AP and 0.5 Gy from the PA to a 12 cm depth, the entrance doses would be about 2.5 Gy. The exit doses would be about 0.1 Gy. So in the neighborhood of 2.5-3.0 Gy on the skin. More interesting to me would be the doses in the lung as the x-rays enter and travel to the midplane prescription point. But even with 6 MV x-rays AP/PA, the pleural surface entrance doses will be twice that of the prescription dose. Really the ideal energy if you want to be more homogenous would be >20 MV x-rays; of course one could say this about any AP/PA prescription in radiotherapy.What would the skin dose be if tried to deliver 1 gy whole lung with ortho voltage?
You'd never know from the tweet that 20% of the radiation treated group died, compared to 0% of controls.
Just learned that olive oil industry is full of fraud. Apparently high end olive oil should have slightly burn on back of palate.I was at the local grocery store and saw "EXTRA Virgin Olive Oil" for $7.50/Liter.
I got so excited and bought it.
Normally, it is $20-$30/L for this extra virgin stuff.
Only after I got home, then I realized it is ONLY 20% Extra Virgin Olive Oil, the rest (80%) is Sunflower Oil...lol.
The 20% Olive Oil is written in small font below the big letter of "EXTRA Virgin Olive Oil".
Live and learn, I guess I can fry some chicken with this oil...not good enough for salad dressing lol...
So, people, read the "small fonts" when reading a scientific article of RT vs Covid...
Don't get me wrong, I love science and I am all for clinical trials, even with RT to lung for Covid.
But I don't like it when the data is being massaged...
The author of that article sure has seen some scary lookin' d***s.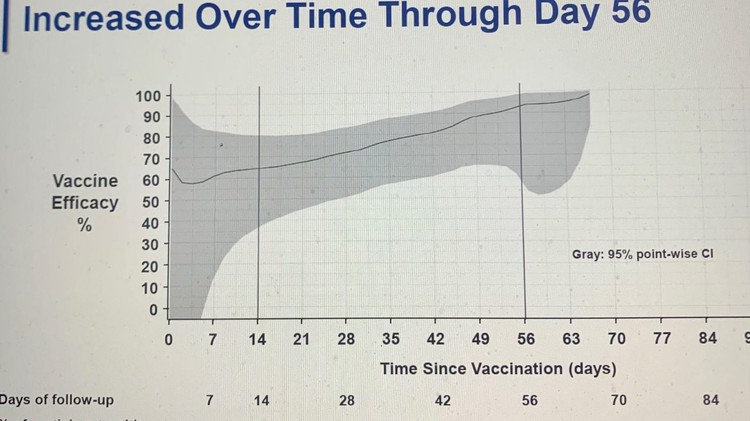
Great News: Johnson & Johnson Vaccine Chart Looks Like a Dick — VICE
This vaccine efficacy chart from the FDA sure looks familiar.apple.news
The obvious explanation is that they didn’t do it right Need the Emory patented deviceStop the presses!
SDN people publish stuff. Wait. "The Mob" publishes stuff.
Conclusions
Whole-lung LDRT failed to improve clinical outcomes in critically ill patients requiring mechanical ventilation for COVID-19 pneumonia.
All the intensivists are breathing a sigh of relief now that they don't have to freak out over the prospect of devising a workflow to transport intubated patients to a linac vault....Stop the presses!
SDN people publish stuff. Wait. "The Mob" publishes stuff.
Conclusions
Whole-lung LDRT failed to improve clinical outcomes in critically ill patients requiring mechanical ventilation for COVID-19 pneumonia.
Rib sparing IMPT whole-lung radiationJust need to open up the proton trials now.
I’m going to patent my SIB IGRT-IMPT DIBH dragonfly technique. Keep 0.03 cc of rib less than 0.001 cGy to avoid 0% risk of long term toxicity in 100 years.Rib sparing IMPT whole-lung radiation
Ralph would be proud of you.I’m going to patent my SIB IGRT-IMPT DIBH dragonfly technique. Keep 0.03 cc of rib less than 0.001 cGy to avoid 0% risk of long term toxicity in 100 years.
