ongoing trial
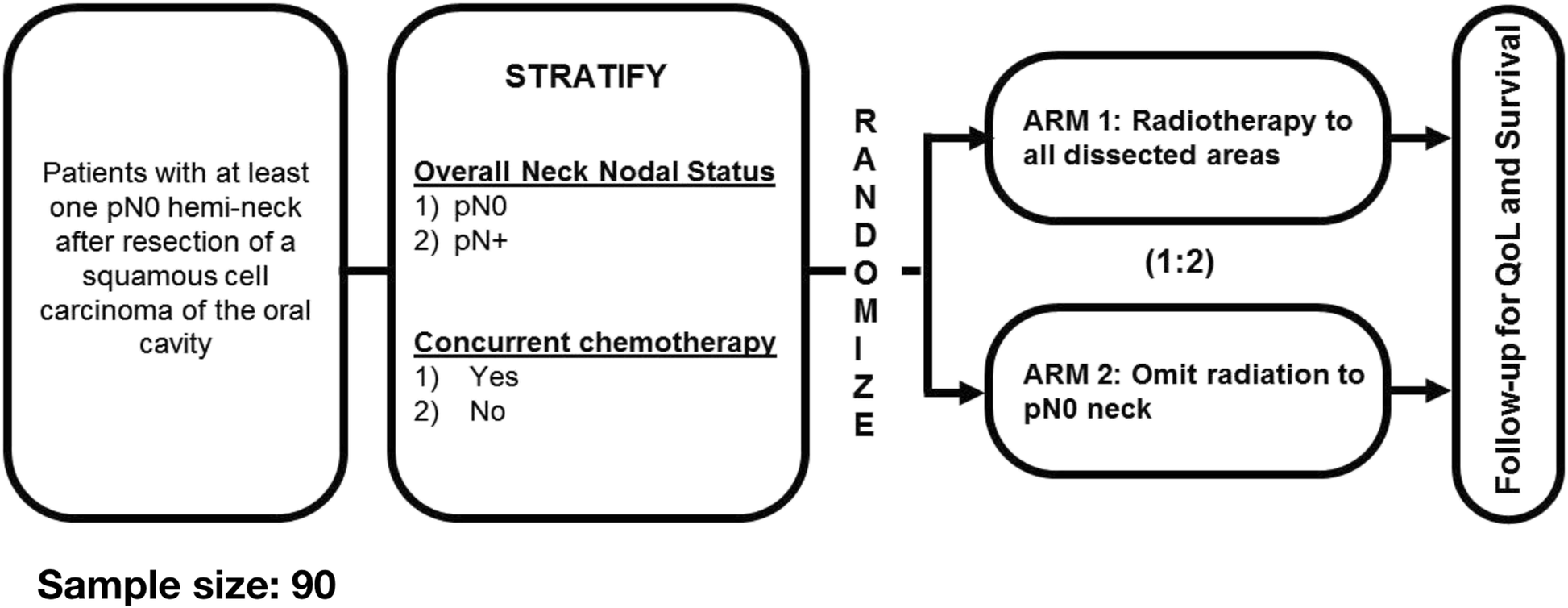
Background Patients with resected oral cavity squamous cell carcinoma (OCSCC) are often treated with adjuvant radiation (RT) ± concomitant chemotherapy based on pathological findings. Standard RT volumes include all surgically dissected areas, including the tumour bed and dissected neck. RT has...

ro-journal.biomedcentral.com
but I'm pretty sure you agree with palma - we need more in HN. every other disease site has multiple.
Of course I do, that was the bloody point! I was being ironic, because „more“ sounded like if we had done ANY AT ALL…
„Every other site has multiple“ is rather exaggerated.
Look at the prostate-lymphatics-mess: One French trial (flawed), one RTOG 9413 (total mess due to 2x2 design), one POP-RT (rather small and somehow too good to be true). And it took us… 30 years to run those trials. In prostate cancer. To us prostate cancer is what hips protheses are to ortho.
But what randomized trials did we do in H&N cancer?
Dozens of trials on chemotherapy - most of them useful, indeed
Dozens of trials on radioprotectors, radiosensetizers (not chemo) - most of them useless
Dozens of trials of fractionation - now, that‘s a tricky one, many useless however.
In this thread, 3 trials were raised on „volumes“.
One was an ancient one showing us how to shield the hypothalamus in nasopharyngeal carcinoma RT - not quite a volumes trial
The other two was on how to spare the swallowing tract and the parotids- also not volumes trials.
These are rather „techniques“ trials.
What I am asking are trials like…
“Do we need bilateral irradiation in N0 supralaryngeal cancer & non-tonsil oropharyngeal cancer?“




")