I'll give it a shot as well.
Minute ventilation = Tidal volume x RR
Your body will try to keep minute ventilation constant at all times (in other words, if the tidal volume decreases, the respiratory rate will have to be increased, whereas if the respiratory rate decreases, the tidal volume will have to be increased).
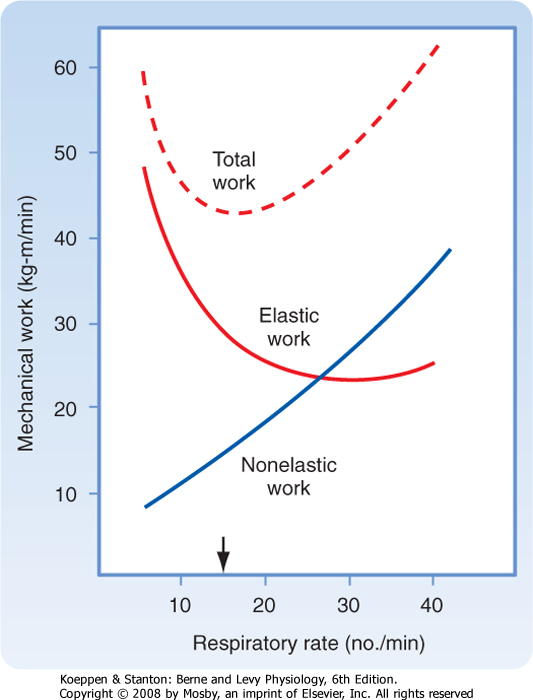
Under normal (i.e., non-pathologic) conditions, your respiratory rate will be ~15 rpm (the arrow on the graph) since it ensures an adequate minute ventilation where total work is minimal.
In cases of restrictive lung disease, compliance is decreased and elasticity is increased, which makes it 1) harder for the lungs to expand/fill and 2) easier for them to empty (in cases of fibrosis, where fibrotic tissue keeps the airways open because of increased radial traction). Making it harder for the lungs to expand means more work is spent when trying to inspire higher volumes (the lung is not being compliant!) so the body will adapt by increasing the respiratory rate (fast, shallow respiration).
In cases of obstructive lung disease, compliance is increased and elasticity is decreased, which makes it 1) easier for the lungs to expand/fill (in comparison to restrictive lung disease) and 2) much harder for them to empty (no elasticity to kick air out!) so the body will adapt by increasing tidal volume (slow, deep respiration).