
group_theory
EX-TER-MIN-ATE!'
Staff member
Administrator
Volunteer Staff
Lifetime Donor
20+ Year Member
- Joined
- Oct 2, 2002
- Messages
- 4,840
- Reaction score
- 2,206
If you haven't seen these two threads, I think it would be worthwhile to read since the topics covered are not typically taught (or taught well) in medical school or residency but important for all physicians (and physicians in training) to know
How a doctor makes money?
How a doctor makes money (Part II)
For this thread, I thought it would be interesting to review an interesting report that Medscape released.
Young Physician Compensation Report 2017
Medscape: Medscape Access
*Note: Signing up for Medscape may be required to view the entire slideshow
Disclaimer: Neither this author nor SDN is sponsored by Medscape, nor does this post signify endorsement of Medscape by SDN or this author.
Conflict of Interest Statement: I have no actual or potential conflict of interest in relation to this post/presentation.
Their sample size (total physicians) who responded to the online survey was greater than 19200, but the breakdown by specialties who responded wasn't even across the board, which can affect the accuracy. For young physicians (defined younger than 40), the N size is 4100
First, here are the income broken down by specialties for Physicians younger than 40
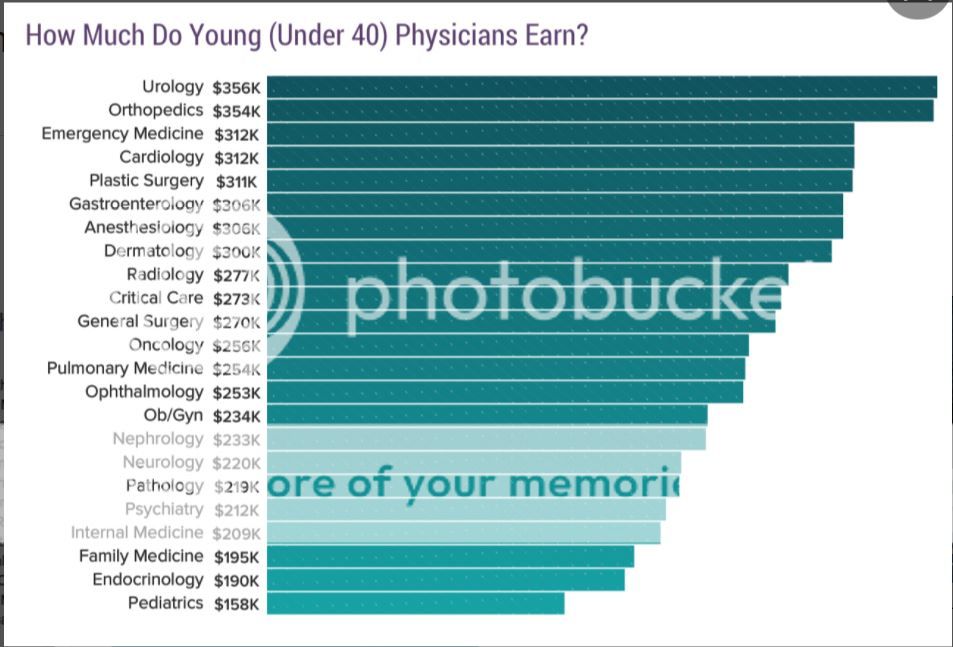
There are certainly a lot of variables that can affect compensation - how many hours a week, the practice environment (Hospital, outpatient, ambulatory surgery center), the employment type (employed/salaried, bonus structure, partnership track), Payor Mix (Medicare? Medicaid? Cash Pay?), as well as procedures/visit types (procedure heavy vs cerebral/office heavy, well-reimbursed procedure vs medicare cuts for reimbursement, etc)
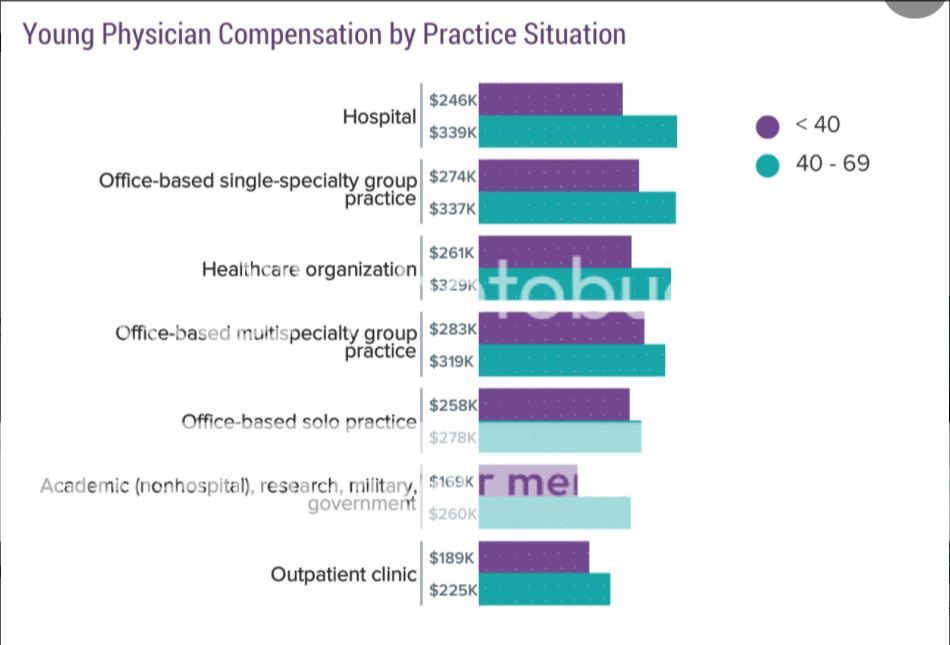
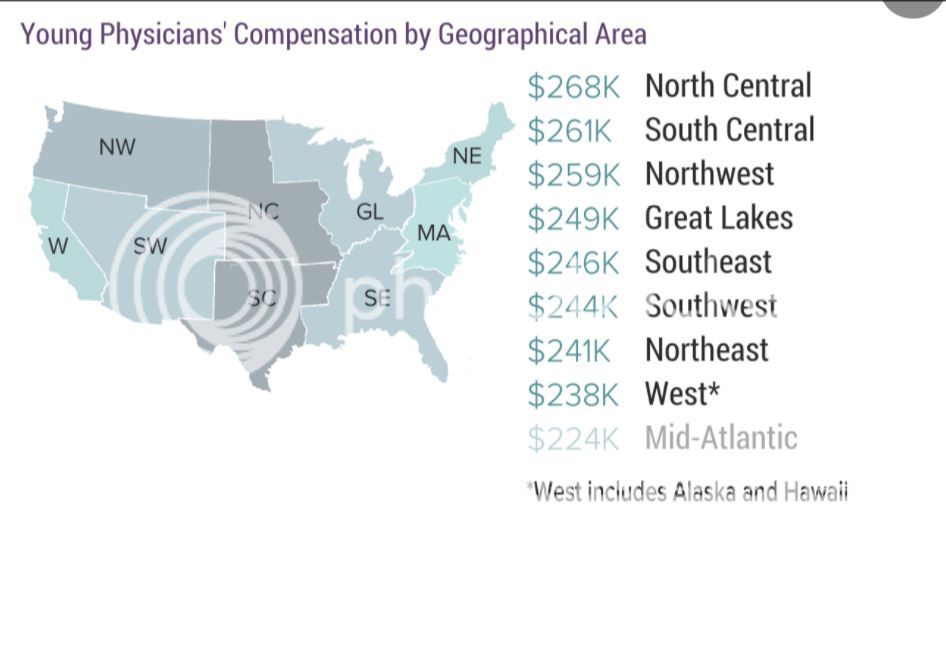
When you are finally done with training and start looking for jobs - you will see that certain region will pay more than others. The general rule of thumb (although not always true) is that you will take a pay cut to work in academic medicine than outside academia (whether your employer is a non-profit hospital, a for-profit hospital, etc). The more prestigious the hospital, often time the bigger the salary hit since it should be an honor to work for such Brand-Named Hospital (however prestige does not pay the bills)
Certain cities will offer a lower starting pay (even though cost of living is higher) due to "demand" - such as SF, Seattle, Manhattan, etc
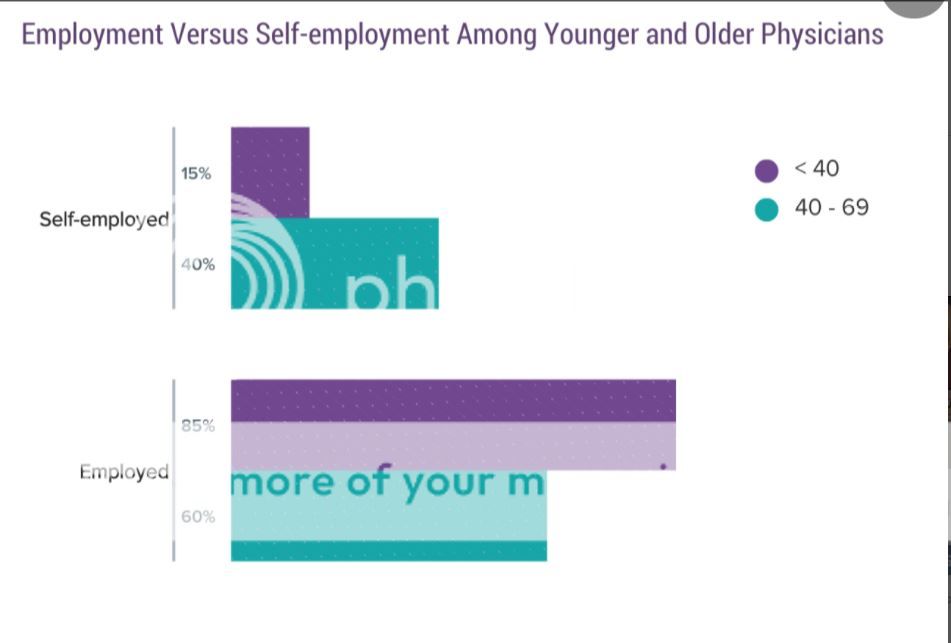
A trend that I find disturbing is that more younger physicians are "employed" than self-employed. While it is certainly easier to be an employee than a business owner (whether single-solo practice, or a partner in a group practice), there will certainly be a direct impact on compensation. If you are a partner in a practice, or solo practice ... your income is that of a small business owner - your compensation is gross receipt minus all expenses. The more you bill (and less outstanding debt/collection), the more you make. For employees, the owners (whether they are the group partners who hire you as an employee/non-partnership track job) or company/corporation - the difference between your compensation and your actual reimbursement goes to the company (whether profit or loss)
It is a lot of headache when you are self employed (in addition to the paperwork and medical decisions related to the practice of medicine - there are business decisions to be made - rent or own? job benefits for your employees? how to keep expenses down?) so it is "easier" to be an employee. There are other benefits (if you are employed by a large healthcare organization, there is a buffer should there be dramatic changes in how physicians are compensated, such as bundled care, or ACO, etc) But being employed comes at a cost.
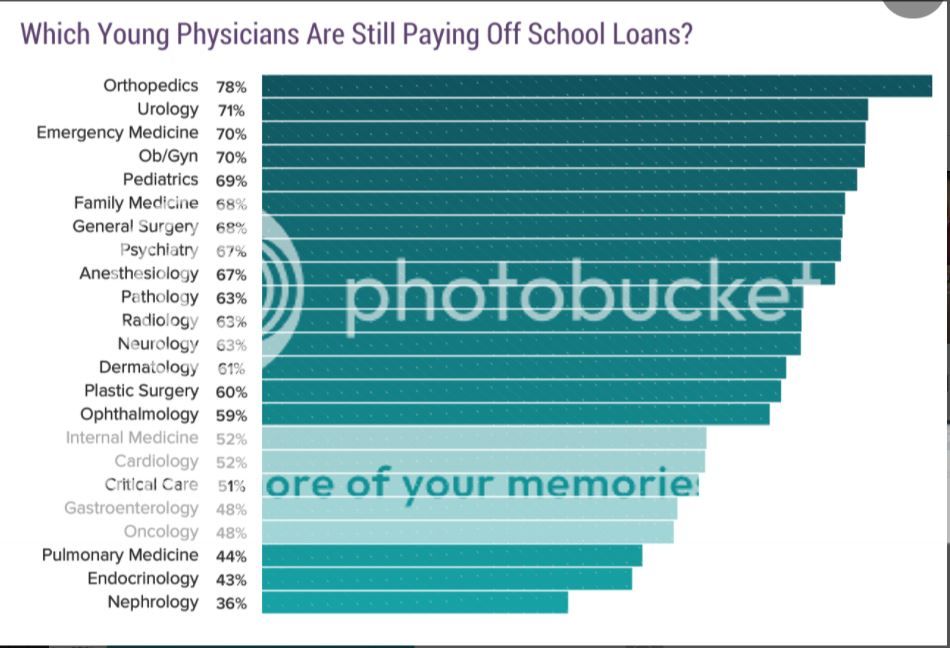
How many are still paying student loans? I can't find a common link between the specialties - it's not related to compensation (ortho and urology are at the top), length of training (emergency medicine, peds, family medicine are 3 year programs), practice environment (EM is hospital, ortho is either hospital or ambulatory surgery center, peds is mostly outpatient), etc.
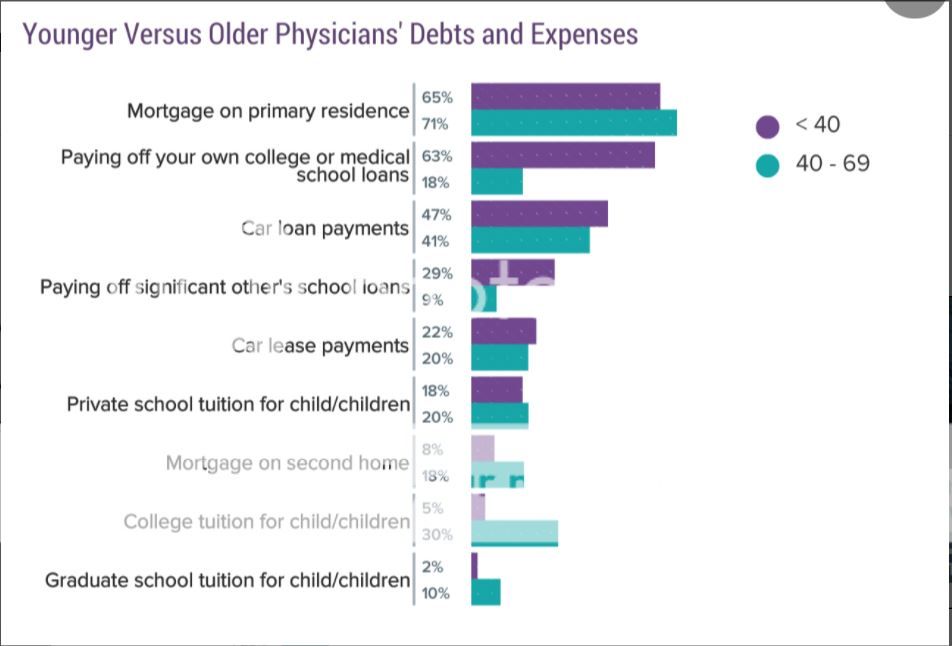
So once you're done with training - there are bills to be paid. What are your expenses?
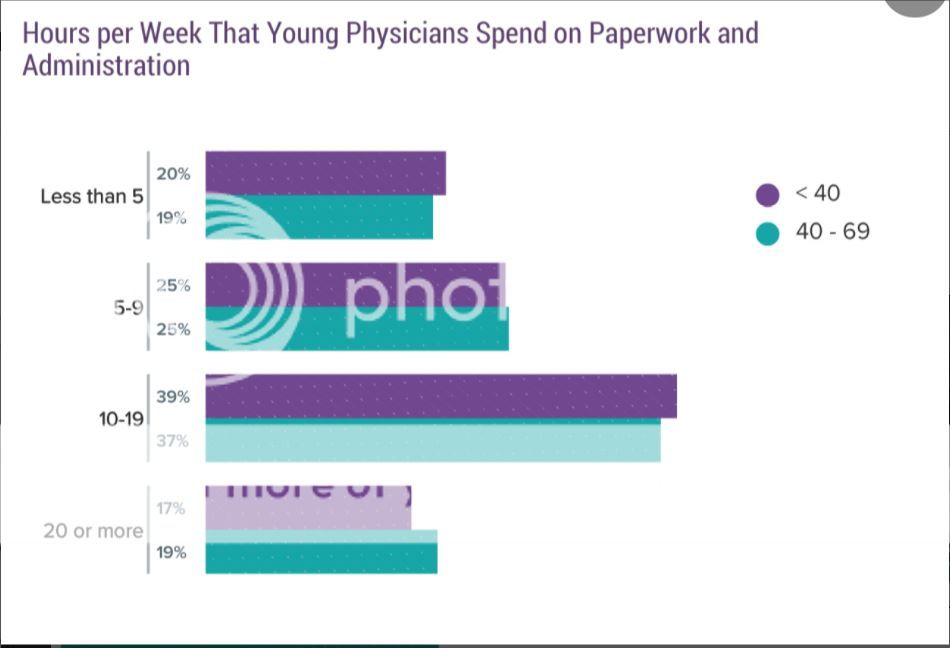
One thing they don't tell you, and you don't realize until you are done with training, is the amount of paperwork and administrative stuff you have to do. If employed by the hospital, they expect you to serve (uncompensated) on various hospital committees as part of your professional obligations. (and to be honest, if your goal is to be a hospital physician administrator such as chief medical officer, etc - you need to make connections and participate/chair various hospital committees as well as make connections/contact with other departments in the hospital such as nursing admin, pharmacy, etc)
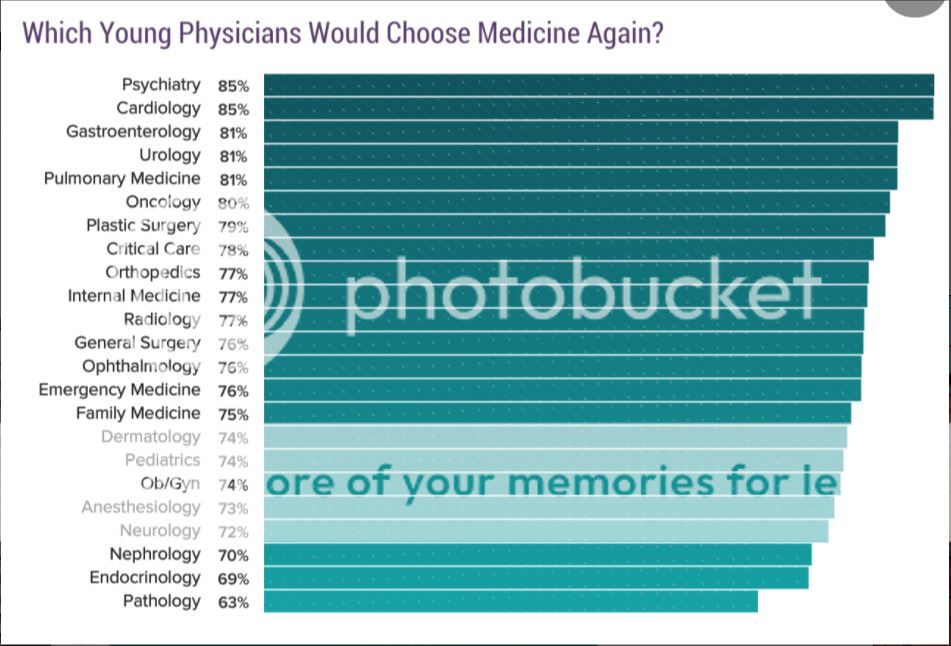
But in the end, was it worth it? Most say yes
How a doctor makes money?
How a doctor makes money (Part II)
For this thread, I thought it would be interesting to review an interesting report that Medscape released.
Young Physician Compensation Report 2017
Medscape: Medscape Access
*Note: Signing up for Medscape may be required to view the entire slideshow
Disclaimer: Neither this author nor SDN is sponsored by Medscape, nor does this post signify endorsement of Medscape by SDN or this author.
Conflict of Interest Statement: I have no actual or potential conflict of interest in relation to this post/presentation.
Their sample size (total physicians) who responded to the online survey was greater than 19200, but the breakdown by specialties who responded wasn't even across the board, which can affect the accuracy. For young physicians (defined younger than 40), the N size is 4100
First, here are the income broken down by specialties for Physicians younger than 40
There are certainly a lot of variables that can affect compensation - how many hours a week, the practice environment (Hospital, outpatient, ambulatory surgery center), the employment type (employed/salaried, bonus structure, partnership track), Payor Mix (Medicare? Medicaid? Cash Pay?), as well as procedures/visit types (procedure heavy vs cerebral/office heavy, well-reimbursed procedure vs medicare cuts for reimbursement, etc)
When you are finally done with training and start looking for jobs - you will see that certain region will pay more than others. The general rule of thumb (although not always true) is that you will take a pay cut to work in academic medicine than outside academia (whether your employer is a non-profit hospital, a for-profit hospital, etc). The more prestigious the hospital, often time the bigger the salary hit since it should be an honor to work for such Brand-Named Hospital (however prestige does not pay the bills)
Certain cities will offer a lower starting pay (even though cost of living is higher) due to "demand" - such as SF, Seattle, Manhattan, etc
A trend that I find disturbing is that more younger physicians are "employed" than self-employed. While it is certainly easier to be an employee than a business owner (whether single-solo practice, or a partner in a group practice), there will certainly be a direct impact on compensation. If you are a partner in a practice, or solo practice ... your income is that of a small business owner - your compensation is gross receipt minus all expenses. The more you bill (and less outstanding debt/collection), the more you make. For employees, the owners (whether they are the group partners who hire you as an employee/non-partnership track job) or company/corporation - the difference between your compensation and your actual reimbursement goes to the company (whether profit or loss)
It is a lot of headache when you are self employed (in addition to the paperwork and medical decisions related to the practice of medicine - there are business decisions to be made - rent or own? job benefits for your employees? how to keep expenses down?) so it is "easier" to be an employee. There are other benefits (if you are employed by a large healthcare organization, there is a buffer should there be dramatic changes in how physicians are compensated, such as bundled care, or ACO, etc) But being employed comes at a cost.
How many are still paying student loans? I can't find a common link between the specialties - it's not related to compensation (ortho and urology are at the top), length of training (emergency medicine, peds, family medicine are 3 year programs), practice environment (EM is hospital, ortho is either hospital or ambulatory surgery center, peds is mostly outpatient), etc.
So once you're done with training - there are bills to be paid. What are your expenses?
One thing they don't tell you, and you don't realize until you are done with training, is the amount of paperwork and administrative stuff you have to do. If employed by the hospital, they expect you to serve (uncompensated) on various hospital committees as part of your professional obligations. (and to be honest, if your goal is to be a hospital physician administrator such as chief medical officer, etc - you need to make connections and participate/chair various hospital committees as well as make connections/contact with other departments in the hospital such as nursing admin, pharmacy, etc)
But in the end, was it worth it? Most say yes
") I agree about avoiding salary, it will be my number one goal, I want a straight RVU based compensation. It may be low the first 6 months to a year, but I am sure it will work just fine after that.
I agree about avoiding salary, it will be my number one goal, I want a straight RVU based compensation. It may be low the first 6 months to a year, but I am sure it will work just fine after that.