Considering the success rate of the H-1B lottery is down to about 1 in 4, I'm curious to see how many employers will find this worth their time.
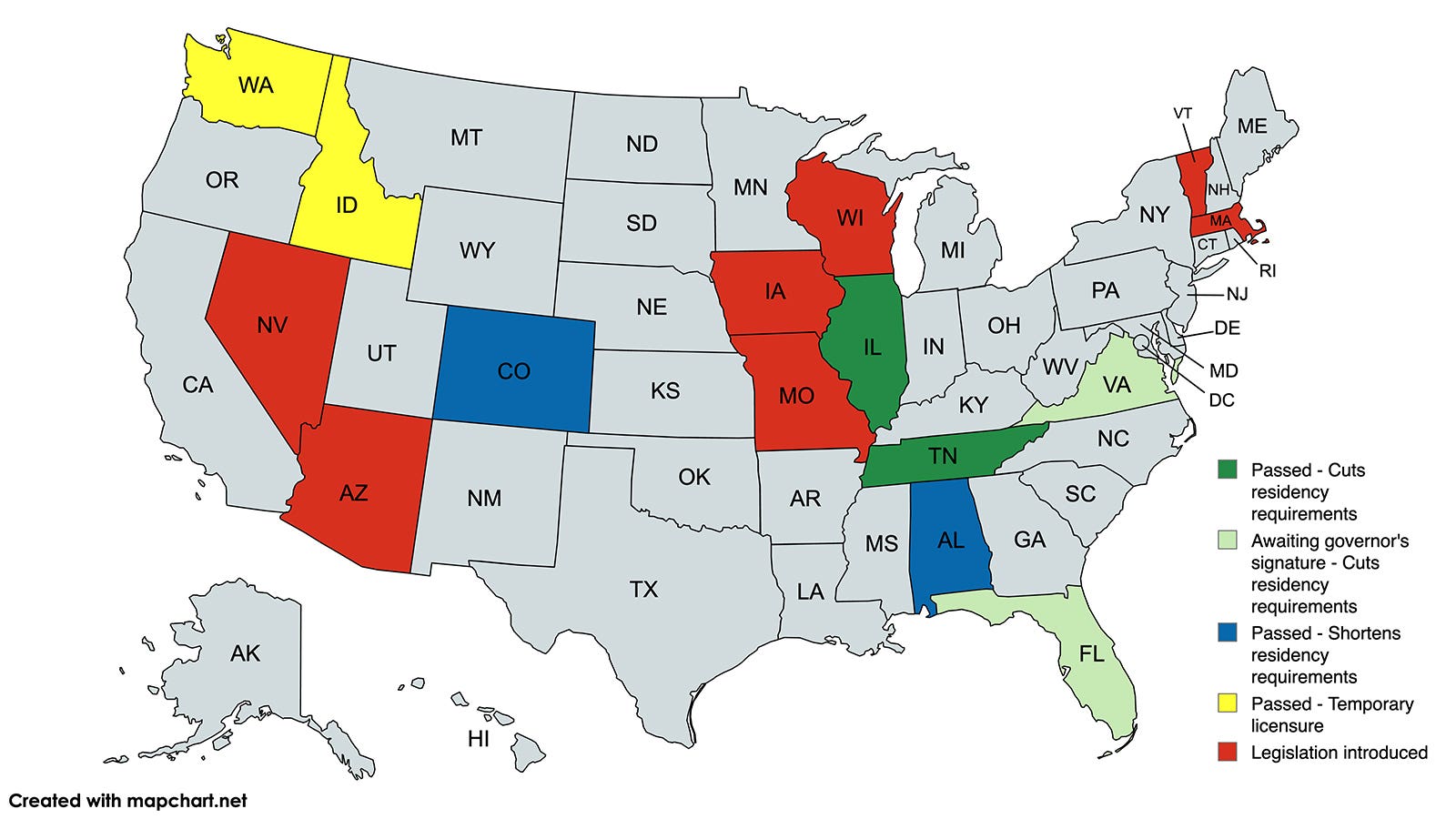
The TN law stipulates that the employer must be operating at least one ACGME-approved training program. Right now there are 9 potential employers with continuing accreditation and 3 with initial accreditation.
I agree, I think the impact will be fairly limited.
As you point out, many of the laws require the employer operate an ACME-approved program. Some require a few years of supervision (sounds almost like a residency...). For states where this isn't a requirement, the hospital is going to have zero idea about whether or not the medical school/residency program the applicant graduated from is decent, and more likely to say the effort isn't worth the risk of a bad physician (bad docs can be very hard to remove for medical staff.
Really bad docs aren't). As a member of our hospital's medical executive committee, there's no way I would approve a foreign-trained physician without any US training/experience unless another member of the committee of a
very trusted/respected staff physician could personally vouch for their skill/competence/ability to communicate/work with the US system.
Realistically we should be more worried about midlevels and AI. Which I don't think we need to be as worried about as people are on SDN--we're in such short supply and patients almost always prefer us when they have a choice (which they unfortunately often don't). The NP industry seems to think just throwing more NPs out into the wild is the answer rather than focusing on quality. They need a Flexnor Report moment or trust/respect of NPs will likely start taking in the next 10-20 years. PA's unfortunately are becoming less relevant because while they serve their role as a physician extender much better, in my opinion, employers want to hire NPs because they're more flexible due to their far more aggressive lobbying.
MD/DO's also need to work on admitting/training more physicians. We're part of the problem. My wife's PCP's office called my wife to cancel her appointment because the doc was going to be on vacation. This is for an annual exam appointment scheduled 6 months prior. And the next available appointment they could offer her despite it being their error, was in another 6 months. 6 months! To say we're short PCPs here is an understatment.
The sky is still here. But AI will likely change our workflow in the next 10-15 years. Maybe longer. Think about how long it took for the digital revolution to finally result in near-universal EMR access.