Interesting. For some reason I'd always pictured it as a focally collapsed lung (like you'd see in pneumothorax) until a UW question showed an image of it
No air and increased tissue density. That's why it's helpful to get an expiratory film when you suspect foreign body aspiration--the side with foreign body will have trapped air and thus be hyperlucent (at least according to Felson's).
No air and increased tissue density. That's why it's helpful to get an expiratory film when you suspect foreign body aspiration--the side with foreign body will have trapped air and thus be hyperlucent (at least according to Felson's).
This confused me a lot so I had to look it up. Apparently kids more frequently get air trapping (which would present with the hyperlucency you describe) while adults tend to get atelectasis. Atelectasis also often doesn't show up until >24 hr post aspiration
This confused me a lot so I had to look it up. Apparently kids more frequently get air trapping (which would present with the hyperlucency you describe) while adults tend to get atelectasis. Atelectasis also often doesn't show up until >24 hr post aspiration
The atelectasis you describe in adults is called absorption atelectasis. Basically, all the air distal to the obstruction gets reabsorbed and the alveoli collapse, because the total pressure of gases in the alveoli equilibrates with the total pressure of gases in the pulmonary capillaries. Normally, nitrogen--which doesn't equilibrate very well--acts as a kind of gaseous "stent," keeping the alveoli open while O2 and CO2 equilibrate. But given enough time, even the nitrogen gets reabsorbed.
This is why, by the way, 100% O2 can sometimes cause absorption atelectasis--because there's no nitrogenous stent keeping the alveoli open as the O2/CO2 equilibrate.
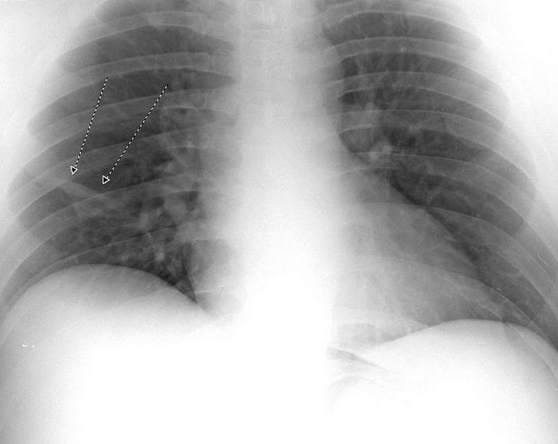
There aren't any signs specific to atelectasis on that CXR, but a hyperdense right side combined with tracheal deviation to the right (indicating volume loss) is well explained by atelectasis
Atelectasis in post-surgical patients who aren't breathing deeply enough to inflate their entire lungs (either due to sedation, pain, or position) can be described as linear, plate-like, or subsegmental and is often in the lower lobes:
This is why, by the way, 100% O2 can sometimes cause absorption atelectasis--because there's no nitrogenous stent keeping the alveoli open as the O2/CO2 equilibrate.
There aren't any signs specific to atelectasis on that CXR, but a hyperdense right side combined with tracheal deviation to the right (indicating volume loss) is well explained by atelectasis
Yeah, I completely missed the tracheal deviation on the UW question. I thought from the image I was looking at a pleural effusion (the density that was actually the atelectasis) with the lucency being the collapsed lung (which was actually the deviated trachea)
I'm not quoting your second post. Too much info, do not want, do not want, :|
The nearly atmospheric partial pressure of N2 in plasma makes the diffusion rate very low, because there's almost no pressure gradient to drive diffusion. But given enough time...
This a great thread! I hadn't thought about the tracheal deviation either.