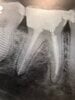
So I am about to prep my first crown in clinic. This wont be an easy one. The tooth is #30 and it has a composite core that goes pretty far subgingival on the distal. I am putting a CEREC long term provisional on this tooth because it will need crown lengthening and the patient still has a lot of phase 1 treatment that has yet to be rendered. Of course the whole margin that this CEREC crown will be sitting on needs to be sound tooth structure (no composite), so I'm going to have to extend the distal margin pretty far below the FGM. From what I can tell from the radiographs I've got about 1.5 mm of natural tooth structure above the bone on the distal aspect. I'm just looking for some advice that anyone might have to make my first crown prep go as smooth as possible. Which size of retraction cords would you pack and what other advice might you have for visualizing and preparing this distal margin the right way? Thanks in advance!
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Crown Prep before crown lengthening procedure, advice needed
- Thread starter TXftw
- Start date

- Joined
- Jul 21, 2004
- Messages
- 1,581
- Reaction score
- 2,505
Do you have any radiographs or clinical photos? I can go into more detail later.
- Joined
- Aug 20, 2006
- Messages
- 3,923
- Reaction score
- 1,248
In the real world, it is possible to have part of the crown margin on composite. If you're talking about a half mm on the distal which would otherwise mean crown lengthening, many do "margin elevation" procedures and put the margin partially/slightly on composite.

In the real world, it is possible to have part of the crown margin on composite. If you're talking about a half mm on the distal which would otherwise mean crown lengthening, many do "margin elevation" procedures and put the margin partially/slightly on composite.
I wish we could do this, but my school they never allow us to put the margin of a crown on anything but natural tooth structure. They're very strict about this rule.
- Joined
- Jun 3, 2009
- Messages
- 2,001
- Reaction score
- 948
Man, that’s a hell of a first crown. Some old school advice would be to place an amalgam core to help visualize that distal margin. An opaque resin core works too but you’ll be battling through a good bit of heme and amalgam is just easier to see. Not sure if your school even uses amalgam though... You have access to any radiosurge/lazers/electrosurgery units for hemostasis? Those are great for tissue and heme management.
Amalgam wasn't an option, they only let us use amalgam for core buildups if the tooth is deemed impossible to properly isolate. I would've loved to use amalgam. I'll likely be taking a lot of radiographs to make sure I'm completely off composite since I know that I am not going to be able to tell clinically. I do have access to a lazer unit and I plan to use it.
This would have been a good opportunity to do a bonded endocrown. You most likely could have avoided crown lengthening and preserved more tooth structure.
Dental school is really a struggle. one tip is to Infiltrate the gingiva for heme control as necessary.
Dental school is really a struggle. one tip is to Infiltrate the gingiva for heme control as necessary.
- Joined
- Jul 21, 2004
- Messages
- 1,581
- Reaction score
- 2,505
So I am about to prep my first crown in clinic. This wont be an easy one. The tooth is #30 and it has a composite core that goes pretty far subgingival on the distal. I am putting a CEREC long term provisional on this tooth because it will need crown lengthening and the patient still has a lot of phase 1 treatment that has yet to be rendered. Of course the whole margin that this CEREC crown will be sitting on needs to be sound tooth structure (no composite), so I'm going to have to extend the distal margin pretty far below the FGM. From what I can tell from the radiographs I've got about 1.5 mm of natural tooth structure above the bone on the distal aspect. I'm just looking for some advice that anyone might have to make my first crown prep go as smooth as possible. Which size of retraction cords would you pack and what other advice might you have for visualizing and preparing this distal margin the right way? Thanks in advance!
A few questions:
- How many walls do you have left intact? If you have 1 or 2 walls left, you may require a post in the distal canal.
- Do you have access to a laser or electrosurge? You can avoid packing cord if you use a laser/electrosurge. Deep margins are the enemy of the CEREC. Trying to visualize a deep margin on the CEREC that's really close to alveolar bone is difficult without significant gingivo/alveoloplasty.
How would you go about capturing the distal margin?
0a (I forgot to add a step, I didn't feel like changing the number system): Pre-scan with CEREC (More on this later), erase the tooth you're going to prep
1. Prep the tooth to your specifications. Ideally, you should be on tooth structure.
2. Use a surgical length round bur (6 or 8), remove all the gingiva that's in your way in the distal. Don't worry, it's in the posterior and it will grow back. Do not use water/high speed at maximum power! - you're going to use the friction/heat generated by the surgical bur to cauterize as you cut. The dentinal/build up dust will help in the digital impression.
2a. Can you see the alveolar bone? If you can, you have 2 options: flapless crown lengthening or maintain hemostasis to obtain digital impression.
2b. If you go with flapless crown lengthening, you can use a diamond round bur/hard tissue laser or other diamond burs to remove alveolar bone.
2c. If you cannot do flapless crown lengthening, you will need to obtain hemostasis. Cord packed against alveolar bone is pretty futile, you need hemostasis, and most hemostasis options are very transient.
3. To obtain hemostasis for your final digital impression, you need viscostat, 30G x-short needle with 1:50epi, and maybe a glick with a torch (more on this later).
3a. If your bleeding is coming from gingiva, inject 1:50epi lido into the gingiva where you see bleeding. This gives you about 2 mins to capture the margins from time of injection. If you still get bleeding, place viscostat, place pressure with gauze/comprecaps, give it a minute. If still bleeding, inject more epi into the alveolar bone of the interproximal if that's where the bleeding is coming from; if from the gingiva, you could heat the plugger end of the glick with a torch and cauterize with heat or inject with more epi.
4. You effectively have 1-2 mins to complete your scan (which should be sufficient assuming you have your pre-scan done already).
Edit/Disclaimer: I don't know how dental school works these days, I kinda did what I want in dschool and thankfully did not get kicked out. If any of these techniques are not allowed by your school, use your own discretion and I assume no liability for what may happen.
Last edited:
- Joined
- Apr 1, 2006
- Messages
- 182
- Reaction score
- 319
If you can get another student to assist you with suction, you should be able to prep this without too much difficulty, but scanning for the cerec mill is going to be a struggle.
Would the faculty allow you to make a good traditional temp crown instead? A well-made temp crown can last many months.
If it HAS to be a milled temporary, you could resort to making a PVS quadrant impression of the prep, pour and trim, and scan the model for cerec. Keeping the distal dry long enough to get a good cerec scan is going to be tough, but keeping it from bleeding for the 60sec it takes to get a PVS quad tray seated should be possible.
Tough case! With the distal this deep I personally would do PVS and a zirc crown (vs e.max) 10 times out of 10 here...
Would the faculty allow you to make a good traditional temp crown instead? A well-made temp crown can last many months.
If it HAS to be a milled temporary, you could resort to making a PVS quadrant impression of the prep, pour and trim, and scan the model for cerec. Keeping the distal dry long enough to get a good cerec scan is going to be tough, but keeping it from bleeding for the 60sec it takes to get a PVS quad tray seated should be possible.
Tough case! With the distal this deep I personally would do PVS and a zirc crown (vs e.max) 10 times out of 10 here...
Ok guys I just got this done. For the purpose of reflection and to help out anyone who might come across this thread here’s how it went. Everything prep wise was smooth as can be. #30 is an easy tooth. That distal margin though.... awful. Had the extend very far while keeping the margin contiguous. This was a difficult task. Took a bitewing and made sure I was on natural tooth. Now comes the worst part; packing the retraction cords was hell. I chose to pack a 00 & a 1. Faculty tried to help me but couldn’t get it on that distal margin. There was just so much heme and saliva. Said faculty got frustrated and left. I was deterred but not broken. Injected a lot of local with Epi around that distal margin and put a bunch of viscostat on a cotton roll and jammed it in there to try to keep the heme at bay. It worked ok but was far from ideal. Again I tried packing the 00 cord in and was successful this time. I got the size 1 around most of the tooth but not in the distal margin. Proceeded to wet the 1 cord and remove it. Same with the 00. Used a triple tray with heavy and light body and captured a very mediocre but workable impression.
Last edited:
Next I poured up the impression and scanned it. Milled the cerec long term provisional. Margins seemed ok in the areas I could actually detect with an explorer. I cant really speak on the distal as it was very hard to detect. I was incredibly short on time so didn’t take a final x Ray. The tooth needs crown lengthening anyways and will get a new crown when the 6 weeks of healing are up. After checking the margins/contacts I did occlusal adjustments until the cows came home. Faculty checked and was happy with it, so was the patient. All in all it was a very stressful and time consuming experience. In retrospect I wish I could’ve used a lazer. The only one my school has was occupied. Thank you all for your guidance. This is what these forums should be for, learning and teaching
- Joined
- Jun 3, 2009
- Messages
- 2,001
- Reaction score
- 948
Lol, how professional of your attending faculty. Good job and getting it done regardless. For future reference, if you get stuck with old school cord and PVS, a 000 with 00 stack may work a little better. Pull the 00 and impress with the 000 in the sulcus. I would use that method for very deep margins with heavy heme (plus the viscostat/ local).
- Joined
- May 9, 2014
- Messages
- 1,836
- Reaction score
- 2,757
You handled that well. I can’t believe your faculty ditched you lol.Next I poured up the impression and scanned it. Milled the cerec long term provisional. Margins seemed ok in the areas I could actually detect with an explorer. I cant really speak on the distal as it was very hard to detect. I was incredibly short on time so didn’t take a final x Ray. The tooth needs crown lengthening anyways and will get a new crown when the 6 weeks of healing are up. After checking the margins/contacts I did occlusal adjustments until the cows came home. Faculty checked and was happy with it, so was the patient. All in all it was a very stressful and time consuming experience. In retrospect I wish I could’ve used a lazer. The only one my school has was occupied. Thank you all for your guidance. This is what these forums should be for, learning and teaching
Glad everything worked out.
Similar threads
- Replies
- 3
- Views
- 2K