- Joined
- Apr 11, 2023
- Messages
- 131
- Reaction score
- 94
- Points
- 106
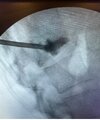
New stat consult for next week. LOL with OP. Severe point tenderness pain apparently in thoracic region. Lateral aspects of the vertebral body are greater heights, but central is pretty squished. About 2mm retropulsion but doesn’t contact the cord on any mri slices.
Would you offer an epidural for palliation, spinejack for fix with lower likelihood of further retropulsion/lower volume of cement, or still try balloon kypho? I am leaning toward spinejack or just vertebroplasty over epidural, last preference would be the balloon. I appreciate any input
Would you offer an epidural for palliation, spinejack for fix with lower likelihood of further retropulsion/lower volume of cement, or still try balloon kypho? I am leaning toward spinejack or just vertebroplasty over epidural, last preference would be the balloon. I appreciate any input