- Joined
- Jan 18, 2013
- Messages
- 155
- Reaction score
- 15
Dear collegues, what do you recommend as an alternative schedule for treating lombar vertebra metastasis ? 5*4 Gy ? 4*5 Gy?
Thank you
Thank you

When are people not doing ap/pa for non-srs palliative spine? What?
How do you define that? I think most people in this day and age contour a volume on a planning CT and critical oar's. Don't see the point of going with anything fancier than appa for someone in severe pain that can barely lay still got 5-10 mins secondary to multi level spinal metsPalex is not in the US so insurers are not telling him what to do (although I think reimbursements are the same no matter what technique you use but I may be wrong ). 2D for bone mets or brain mets is unacceptable in my view. Why not use 3D for field in field (for brain) or multi field bone mets treatment. In think insurers / CMS should have a "simple 3D" code for all palliation and reimburse at an appropriate rate as they do for "simple IMRT".
Sent from my iPhone using SDN mobile
How do you define that? I think most people in this day and age contour a volume on a planning CT and critical oar's. Don't see the point of going with anything fancier than appa for someone in severe pain that can barely lay still got 5-10 mins secondary to multi level spinal mets
Sometimes those multi field plans help and the patient can tolerate the extra table time, in other situations, you want to get them on and off as quickly as possible. I would hope no one is doing "2D" treatment a la slapping fields on an xray and calling it a day.I would think that contouring and prescribing to a volume is 3D. Obviously insurers don't agree.
Using non opposing beams (i.e. Posterior obliques or 3 field to treat a spine) with optimal weighting/beam energy of each beam is not really more time consuming for the patient than APPA. Clearly it is less complex than a 3D definitive plan but more complex than an open field (or simple blocking) APPA or PA 2d plan.
Sent from my iPhone using SDN mobile
Nope, would be considered fraudulent. Upcharging or downcharging a patient is frowned upon.IMRT pays a bit more than 3D here, around 10% more.
Doing ap/pa is not good treatment in my view. It's more toxic, especially for bowel.
I also have the impression of less esophagitis in many IMRT plans nowadays for thoracic vertebral mets.
I'm just curious, but: would the insurer reimburse you for 2D/3D in the US if you did IMRT instead?
Using IMRT for a conventional palliative spine treatment seems pretty out there to me.
AP/PA is pretty darn standard and is what is being done in most academic institutions for non-radiosurgery treatments. Of course you throw blocks on using MLC, so that makes it 3D by definition.
Not sure where you get the idea that AP/PA is toxic?
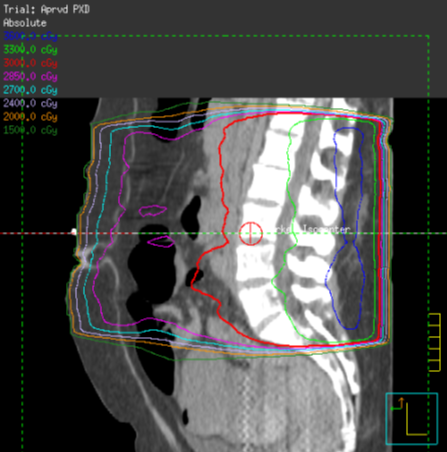
Well if you are going to treat L1-L5 in an obese patient with ap/pa, you are going t have considerable amounts of bowel within the high dose region and dependent on how you weight the fields, this may very well be the 90% isodose the bowel will be in. It will definetely be the 80% isodose.
Here's an example I found online:
This is toxic. It will cause nausea, it will cause diarrhea, it will cause lots of fatigue.
That's my experience.
Around the kidneys, I also use VMAT. In order to protect the kidneys, you can allow two limited arcs (150-210 degrees and 340-20 degrees),it works well.
Oblique fields are also very good, we switcherd to them around 8 years ago instead of ap/pa and then went to VMAT 2 years ago.
Well if you are going to treat L1-L5 in an obese patient with ap/pa, you are going t have considerable amounts of bowel within the high dose region and dependent on how you weight the fields, this may very well be the 90% isodose the bowel will be in. It will definetely be the 80% isodose.
Here's an example I found online:
This is toxic. It will cause nausea, it will cause diarrhea, it will cause lots of fatigue.
That's my experience.
Around the kidneys, I also use VMAT. In order to protect the kidneys, you can allow two limited arcs (150-210 degrees and 340-20 degrees),it works well.
Oblique fields are also very good, we switcherd to them around 8 years ago instead of ap/pa and then went to VMAT 2 years ago.
Correct. Even Medicare, which is arguably the easiest to deal with, does not have bone mets on its general list for imrt approval. I've had denials before from Medicare and had to send in letters of medical necessity because a pt had previous xrt at an adjacent site which is why I didn't do 3D in the first place.How the heck do you get this authorized/approved by insurers?
I can only get AP/PA and believe it or not if performance status is on the lower end I'm starting to get grief for doing 10 fractions (they literally won't even pay for 3Gy x 10 AP/PA and want me to treat 8Gy x 1 to the lumbar spine ... if I tried IMRT or VMAT they would laugh in my face!)
without insulting anyone- we are talking about hypo fractionation here,