As I mentioned before, let us start with the most often cited clinical problem that shows a lack of treatment-by-disorder effect (i.e., lack of differences in treatment efficacy); depression. I teach my students and I tell my friends/family that dozens of treatments are equally efficacious - broadly speaking - in treating depression. This is primarily due to the heterogeneity of the disorder. Now, let us address your second point about mechanisms.
If we don't know the mechanism we are targeting, perhaps its a bit too early to focus on what we need to do to fix the car.
having research identify mechanisms that reliably work and which we can explain/target seems critical. We simply don't have that, so putting specific TXs as standouts seems odd to me because it assumes we know something about those treatments that we don't (i.e., why they work / that they work differently than others).
I'm yet to see studies substantially supporting a specific theory in terms of identifying a single mechanism explanation for anything
Along with that, we have not identified actual mechanisms of change associated with recovery to predict outcomes
There are more but this is enough quoting
Each of our 4 orientations theorizes different etiologies/pathologies and, in turn, different therapeutic mechanisms. I will simply/broadly highlight those mechanisms (let us not nitpick, it is meant to be broad)
Psychodynamic/analytic: unresolved unconscious conflicts; resolved through a relationship with therapist (perhaps the one I understand least?)
Humanistic (and similar): lack of self-actualization; unconditional positive regard
CBT: learning/cognitions create maladaptive behaviors; new learning and new thoughts
Biological/Medication: biological malfunction; alter biology
What I mean by heterogeneity of depression is that depression is caused by a **** TON (damn SDN trying to censor me) of reasons. Numerous pathways to the disorder, numerous pathologies. We know that CT, BT, pyschodynamic, meds, and exercise all have relatively similar efficacy. The problem is that we use these treatments as a panacea. Thus, our relatively small effect sizes (~
d = .24; see Cuijpers article posted above). Here is the crux of the argument:
People get depressed for a myriad of reasons. Daily hassles, existential concerns, social isolation, depressant substances (e.g., certain meds, alcohol), sedentary lifestyles, learned behaviors, maladaptive thoughts, going through a traumatic event, seasonality (I can go on for a long time)). So, it is true that, on average (very broad examinations), will all find similar outcomes. This is due to the dilution of the therapeutic “signal” among the heterogeneous etiologies (“noise”). For example, on average, exercise is as good as most other treatments. However, if I was working with an ultra-marathoner with depression (which I have), the idea that this person is depressed b/c of sedentary lifestyle is asinine. Having this person exercise more will not lead to a therapeutic effect (from the exercise itself, any therapeutic effect can be attributed to other factors [expectations, time, common factors, etc.]). So, comparing a sample of people with heterogenous pathologies that lead to depression across treatments will obfuscate the effect of any individual treatment. More specifically, if I have a trial of exercise for depression but my sample consists of a mix of etiologies (e.g., existential concerns as the main cause for depression plus sedentary folks, and those that consume too many depressants), the effect of exercise, overall, will be decreased. This is an example that some treatments are indeed better than others (theoretically) if we were able to parse out the etiological differences (I don’t think anyone is doing this kind of work). Simply speaking, exercise is great for depression but not for people who are depressed and already exercise a lot. That subset of people likely needs to use a different treatment after understanding the cause of their depression (maybe social, maybe existential).
Now let us look at a less heterogenous disorder, anorexia. We can safely conclude there isn’t a single pathology for anorexia, but it is definitely less heterogenous (or more homogenous) than depression (theoretically). Since there are fewer potential pathologies, then we should be able to see fewer effective treatments (that rely on those theoretical pathologies). Lo and behold, there is no medication (or other biological intervention) that will change a person’s eating behavior (this is not to say that there is no biological component to anorexia, only that any biological component is superseded by an alternative pathology). What works best? Family Therapy (a term often used broadly for any treatments incorporating families but, in this case, a specific treatment for youths with AN).
LINK 1
LINK 2
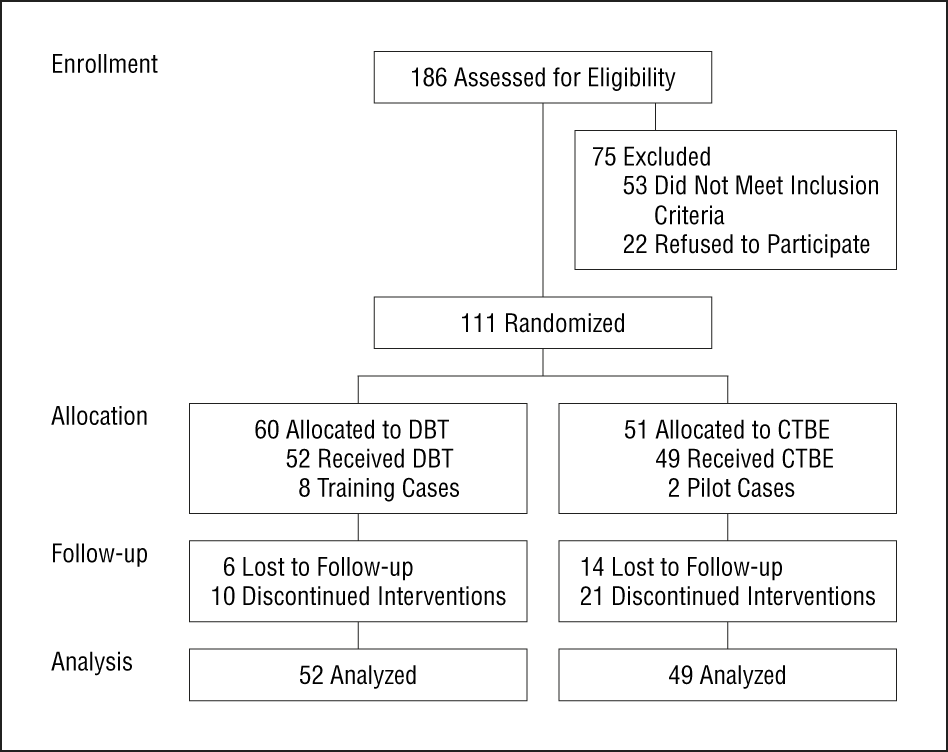
Adults with AN, nothing is great for adults. But for bulimia, we do have some evidence that certain treatments are worse. For example, Lilienfeld discusses Poulsen et al. (2014), which was an RCT that stacked the odds toward a psychoanalytic treatment. Yet, the results very heavily in favor of CBT.
The research on etiologies for disorders is poor for a few reasons. Mainly, we cannot do RCTs for what causes anorexia (or any disorder), that would be blatantly unethical. Furthermore, these need to be longitudinal studies, which are very costly. We often must infer etiological causality. But we can definitely rule out some theories (e.g., no support for the chemical imbalance/serotonin theory of depression; 5-HT transporter gene theory has been debunked;
Collaborative meta-analysis finds no evidence of a strong interaction between stress and 5-HTTLPR genotype contributing to the development of depression).
You further point out that any treatment difference is an anomaly rather than the rule. So far, I have outlined that this isn’t true for youth AN and BN. Similarly, I already highlighted that this isn’t true for multi-problematic suicidal individuals (youth and adult). For depression, this is a consequence of heterogeneity of etiologies. Let us move onto (hopefully our last set of disorders), anxiety.
Still more, have I lost everybody now?



:")