TAP: A New Standard for Abdominal Surgery?
Loran Mounir Soliman, MD, Cleveland, Ohio
IN THE NEAR FUTURE, NERVE BLOCKS MAY BE AS PREVALENT IN ABDOMINAL SURGERY as they are today in orthopedic surgery. At least that's what our experience here at the Cleveland Clinic indicates. For two years, we have been performing transversus abdominus plane (TAP) blocks for pain control after abdominal surgery. These blocks have been so successful that we now are exploring their use for new different indications in a large percentage of our abdominal surgery cases.
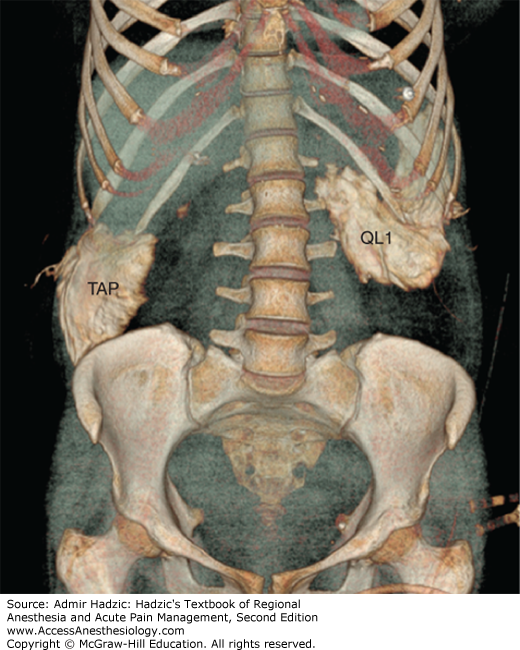
TAP blocks produce a sensory block of the anterior abdominal wall — namely, the lower six thoracic and upper lumbar abdominal afferents. Just like peripheral nerve blocks, TAP blocks effectively control pain, reducing the need for opioids and related side effects like drowsiness and PONV. These patients also typically do not require epidurals, so we also avoid side effects like urinary retention, hypotension, and delayed ambulation due to compromised lower extremity motor function.
Our first foray into TAP blocks consisted of single-shot blocks for minor procedures like inguinal hernia repair. They were so successful that we soon started using continuous TAP blocks (with indwelling catheters for two to three days) for more extensive procedures like kidney transplants, hysterectomies and colostomy closures.
More recently, we began using TAP blocks to treat chronic post-surgical anterior abdominal wall pain, which can develop in 10%-30% of patients after inguinal hernia repair, cholecystectomy and other laparoscopic procedures due to activation of peripheral sensory neurons or direct nerve injury during surgery. Traditionally, patients with this kind of pain have had to undergo the epidural differential test. However the interpretation of the differential epidural test sometimes is very confusing. It is time consuming (takes few hours) and it carries the limitations and disadvantages of neuroaxial. On the other hand, the TAP block provides near immediate diagnostic feedback, so we can pinpoint the source of the chronic pain much faster.
Ultrasound has been a big factor in our success. Traditionally, TAP block technique was blind; we used a blunt needle and confirmed needle placement by feeling double "pops" as the needle passed through the external and internal oblique muscles and fascia. Now, with ultrasound, we can visualize the different layers of muscle and can see both the needle position and the injection. This has made the technique much more reliable. We still use a blunt needle for the reassuring tactile feedback.
TAP blocks are so effective, and they are easier than ever to administer. If our experience here is any indication, TAP blocks are destined to experience a rapid rise in popularity equivalent to that of peripheral nerve blocks. And that will be a good thing for patients and practitioners.
Reference
Ref: Ultrasound-guided transversus abdominus plan block for the management of abdominal pain: An alternative to differential epidural block. Techniques in Regional Anesthesia and Pain Management, 2009: Volume 13, Issue 3, Pages 117-120 L. Soliman, S. Narouze
Dr. Mounir Soliman is Staff Anesthesiology Section Head for Orthopedic Anesthesia and Director of the Regional Anesthesia Fellowship at the Cleveland Clinic, Cleveland, Ohio.