D
deleted388502
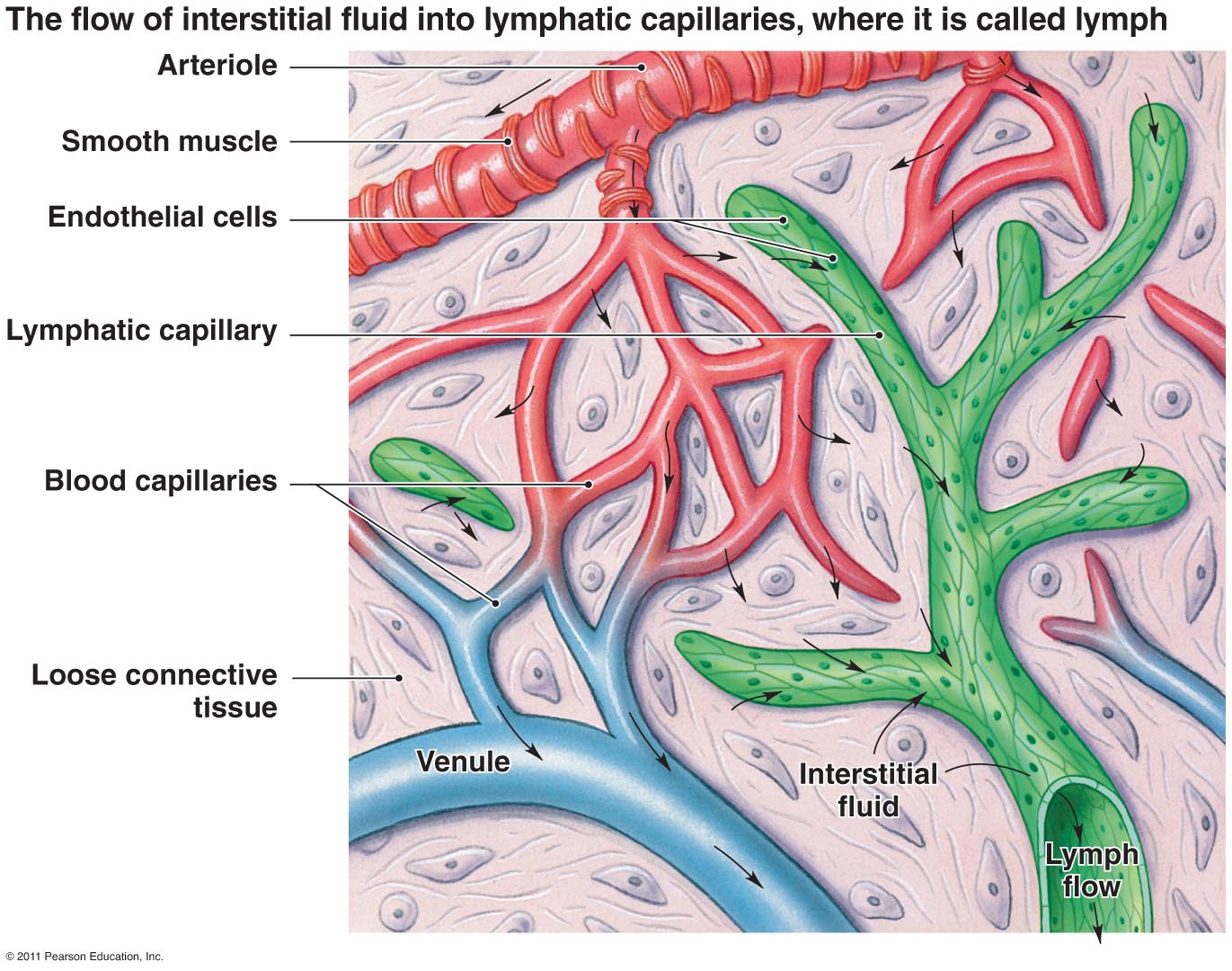
Alrighty so I'm a tad confused on this whole deal with capillaries losing some of the fluid due to osmotic pressure being greater than hydrostatic pressure near venules.
Could someone clear this up? I know the diagram in the EK textbook also shows that 10% is lost to the lymph, and I got a bit lost there - does this just mean that so called "good" nutrients that should be going through the capillaries are lost with the large proteins and other things taken up by the lymphatic system?
I understand that the blood is being pushed from artery --> arteriole --> capillary via hydrostatic pressure, but I don't understand how osmotic pressure is overcoming the hydrostatic pressure near the venule end.
Also, when we say capillaries are the site of nutrient exchange in interstitial tissue - can someone just specify what interstitial tissue is NOT included in this, and what nutrients are not included? I know fat is transported via lacteals and carbohydrates/proteins are taken via capillaries, so does it just include proteins and carbohydrates?
Thanks!
Could someone clear this up? I know the diagram in the EK textbook also shows that 10% is lost to the lymph, and I got a bit lost there - does this just mean that so called "good" nutrients that should be going through the capillaries are lost with the large proteins and other things taken up by the lymphatic system?
I understand that the blood is being pushed from artery --> arteriole --> capillary via hydrostatic pressure, but I don't understand how osmotic pressure is overcoming the hydrostatic pressure near the venule end.
Also, when we say capillaries are the site of nutrient exchange in interstitial tissue - can someone just specify what interstitial tissue is NOT included in this, and what nutrients are not included? I know fat is transported via lacteals and carbohydrates/proteins are taken via capillaries, so does it just include proteins and carbohydrates?
Thanks!
Last edited by a moderator: