- Joined
- Jun 18, 2019
- Messages
- 474
- Reaction score
- 416
anyone know what the job market is like for these other small fields? Especially GynOnc?

Gyn onc produces very few of their own per year. There are only about 750 in the country. I think about this often, especially in the context of cervical cancer. Cervical cancer is by definition a rare cancer, and it's getting rarer and rarer (about 7 per 100,000 and falling) thanks to the HPV vaccine. In rad onc, obviously a big part of our training... and our textbooks, exams, etc... are given to gyn onc, cervical cancer especially. Each one of us can wax eloquently, I'm sure, on the technical minutiae of cervical cancer brachytherapy. There is an implicit demand in rad onc training in the US: thou shalt devote a significant proportion of thy neurons to gyn onc and brachy and the dovetailing of the two.anyone know what the job market is like for these other small fields? Especially GynOnc?
Gyn onc produces very few of their own per year. There are only about 750 in the country. I think about this often, especially in the context of cervical cancer. Cervical cancer is by definition a rare cancer, and it's getting rarer and rarer (about 7 per 100,000 and falling) thanks to the HPV vaccine. In rad onc, obviously a big part of our training... and our textbooks, exams, etc... are given to gyn onc, cervical cancer especially. Each one of us can wax eloquently, I'm sure, on the technical minutiae of cervical cancer brachytherapy. There is an implicit demand in rad onc training in the US: thou shalt devote a significant proportion of thy neurons to gyn onc and brachy and the dovetailing of the two.
Yet now we are facing a "brachy crisis" in the US. Lofty goals to produce 300 competent (why are we devoting training in residency to get competent if we have to get re-competent after residency?) brachytherapists in 10 years have been downsized to 100 in 3 years. (The mathematically savvy will realize 100 in 3 years proportionalizes to 333 in 10 years, so it's really an upsizing; rad oncs: so smart but sometimes so mathematically challenged.) Now why is there a crisis? Why is brachytherapy dying?
We are diluting the brachytherapists (all of us, the rad oncs), and there is also a shrinkage of the gyn onc case load in the US. Et voila. Brachytherapy begins to die because the "average" rad onc is seldom if ever doing brachy nowadays. And please know, the "average rad onc" moniker is not a dis. The "average" should be this: board certified, well trained, healthy, woke, on top of MOC, reading the literature a minimum of 5 hours a week, kind to old people and dogs. The "average" rad onc should be much more than the average human. But math, and one its simple concepts, the "average," affects average rad oncs and average humans alike. There are 5000+ rad oncs in the US, and the number just grew by ~4% this week. (The average number of cervical cancer cases WILL NOT grow by ~4% this year.) There are about 12,000 brachy-able cervical cases in the US a year. For the gyn oncs, this is on average, 16 patients a year. Not a lot, but they're giving chemo, rounding, operating, biopsying, and seeing all the other gyn onc things too. But for the "average" rad onc? He or she will only have access to, on average, 2-3 cervical patients per year. Think about that. And if somebody near the average rad onc is getting more than his average share, then the average rad onc will be seeing zero cervical cancer patients per year. If there's a rad onc seeing 20 cervical cancer patients per year... it means 9 other practicing rad oncs on average are seeing zero per year.
So the cervical cancer and brachytherapy story in rad onc should be a cautionary tale. It shows in a nutshell the demand/supply issues threatening us. It shows that outsize time on learning about cervical cancer and brachy in rad onc residency, as bad as I hate to say it, is dumb. It's not dumb because it's not good knowledge. It's just dumb because it's a rapidly growing waste of time. Which is sad, because if there were half as many rad oncs in America, learning about brachy would be twice as effective for every resident in training. And people would actually be doing brachy after getting out of training. And brachy wouldn't be dying.
Then brachy is not "dying," and I'm wrong. I want to be wrong. We are, however, producing brachytherapists at a positive rate where the indication for some of the brachytherapies is increasing at a negative rate or increasing at a rate much slower than the brachytherapist production rate. About that, I'm not wrong.as a recent grad, I can assure you that the time spent on cervical cancer or brachy education is not as outsized as you seem to think?
I agree and somewhat echoes my point. If it's a "minor" part of what gyn oncs do...Cervical cancer is a minor part of what they do. Most of their day revolves either around hysterectomy volume or chemo/drugs for ovarian cancer.
Fun, true story: when I interviewed as a resident with one D Hallahan (ie to become a resident) our brief convo was basically all about cervical cancer brachy. He wanted to know if I knew what a point A dose was, what T&O's were, and then he launched into a plan wanted me to evaluate the plan, talk in-depth about cervical cancer, etc. That was my whole interview. (Well, he did at the end talk all about the molecules he was developing to make RT work better.) Damnedest thing ever!as a recent grad, I can assure you that the time spent on cervical cancer or brachy education is not as outsized as you seem to think?
Then brachy is not "dying," and I'm wrong. I want to be wrong. We are, however, producing brachytherapists at a positive rate where the indication for some of the brachytherapies is increasing at a negative rate or increasing at a rate much slower than the brachytherapist production rate. About that, I'm not wrong.
Used to, prostate especially. But what the Ivory Tower has blindly and blithely missed is that by increasing the number of rad oncs, it diluted everyone's workload. And thus it makes financially infeasible for most folks, and even hospitals, to maintain a brachy program. Again, one of the "fatalities" in the Rad Onc Oversupply Debacle although no one ever recognizes it or points it out as such. Besides me 🙂do you do brachy in your practice?
Not to mention CMS regs that traditionally didn't allow us to leave the Linac and go to the or to do casesUsed to, prostate especially. But what the Ivory Tower has blindly and blithely missed is that by increasing the number of rad oncs, it diluted everyone's workload. And thus it makes financially infeasible for most folks, and even hospitals, to maintain a brachy program. Again, one of the "fatalities" in the Rad Onc Oversupply Debacle although no one ever recognizes it or points it out as such. Besides me 🙂
anyone know what the job market is like for these other small fields? Especially GynOnc?
Used to, prostate especially. But what the Ivory Tower has blindly and blithely missed is that by increasing the number of rad oncs, it diluted everyone's workload. And thus it makes financially infeasible for most folks, and even hospitals, to maintain a brachy program. Again, one of the "fatalities" in the Rad Onc Oversupply Debacle although no one ever recognizes it or points it out as such. Besides me 🙂
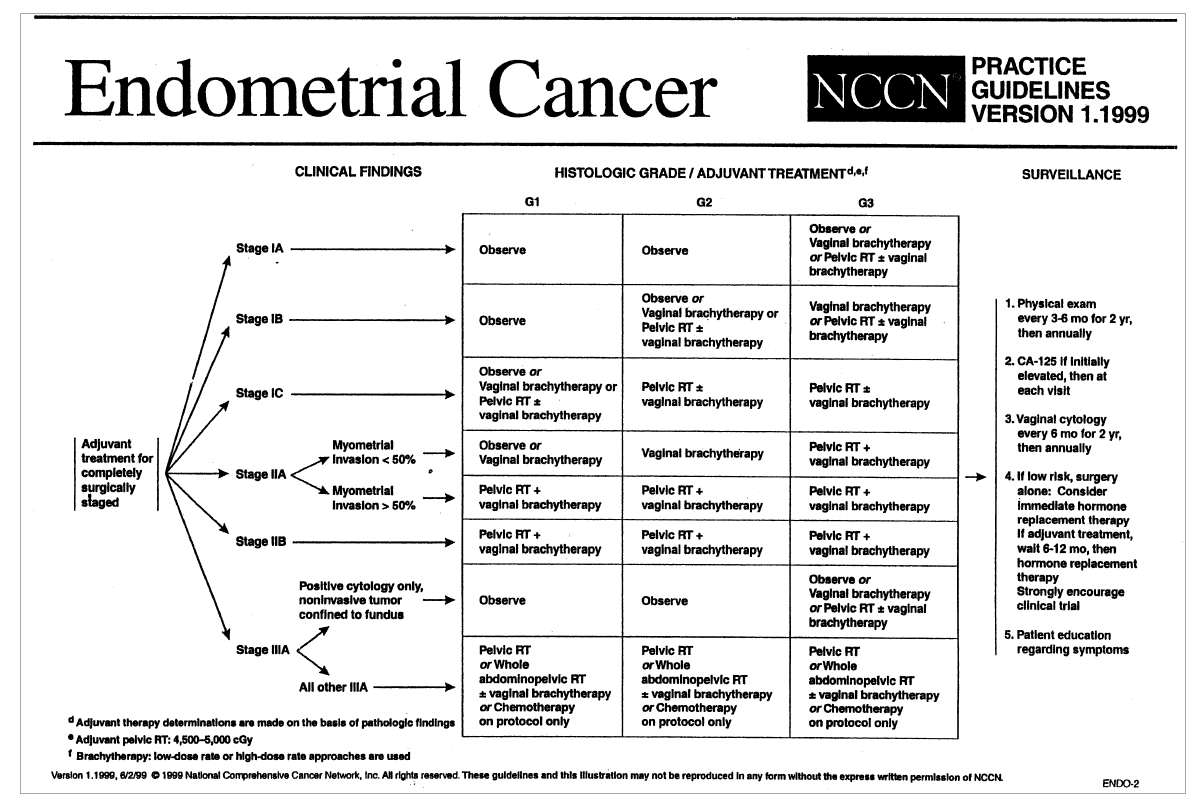
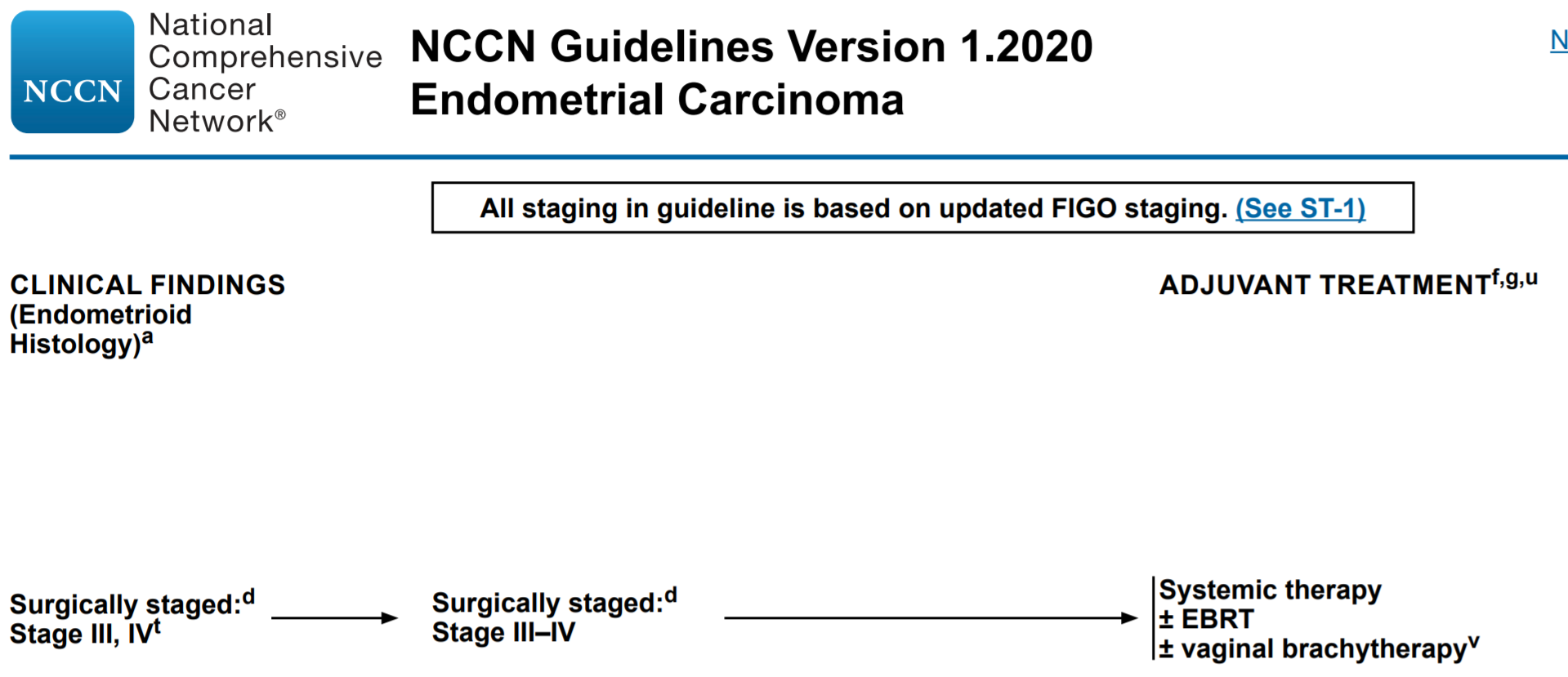
For rad oncs and people interested in becoming rad oncs: so what is the landscape for gyn rad onc now? We are very much more out of the endometrial game than we were 15 or more years ago. Ovarian? Why do we even learn about that in rad onc (but we do)? And cervical? It’s a “small part” of what gyn oncs manage (I agree). (I don’t know if we’d know the name Carlos Perez without cervical cancer though.) And there are about 7 times as many rad oncs as gyn oncs, so it means we manage about 1/7 of their cervical small part! Yikes. And we have a whole oral boards section on gyn rad onc... and most of us will wind up barely practicing it. Thanks, workforce dilution.Also, cervical cancer is a small part of what gyn oncs manage. Endometrial and ovarian are their bread and butter.
We are very much more out of the endometrial game than we were 15 or more years ago.
If you even have access to a referring gyn onc ... ~750 gyn oncs referring to 5000+ rad oncs nationwide... thank goodness American rad onc trainees only have to complete something to the tune of maybe, max, one gyn onc brachy procedure every three months in residency. If we required one every two months or more, there'd simply be too many American residents for the requirements to be met. From a mathematical perspective, we should be hitting up against the 1 every 3 months number soon, I predict, and 1) ACGME will have to lower requirements, 2) programs will have to close, and/or 3) increased case log "fudging" will have to be undertaken.It is very dependent on the practice patterns of your referring gyn oncs.
Afaik the data for RT is still good in dlbcl? The issue, like in some HL pts is whether med onc decides to believe in the data and refer for RT...This is sad but the data support your statement. Many dogmatic gyn-oncs don't believe in adjuvant RT even for node positive patients. GOG has an open post-op trial randomizing to various chemo schemes and no radiation. Where I practice the updated PORTEC-3 results have stemmed the tide against chemo-only for stage 3 patients. In fact, because of GOG49 we are still radiating some of the high-risk early stage patients as well. The similarities between endometrial and DLBCL are eerie. As the data showing the benefit to adjuvant RT gets better, global utilization goes down 🙁
All that being said, I there are a lot of us with a Gyn Focus and very high patient volumes. It is very dependent on the practice patterns of your referring gyn oncs.
Afaik the data for RT is still good in dlbcl? The issue, like in some HL pts is whether med onc decides to believe in the data and refer for RT...
Endometrial cancer, a 20 year evolution:The data is great. That is my point. Utilization is going down despite positive results. Data be damned.