- Joined
- Dec 4, 2011
- Messages
- 1,848
- Reaction score
- 2,515
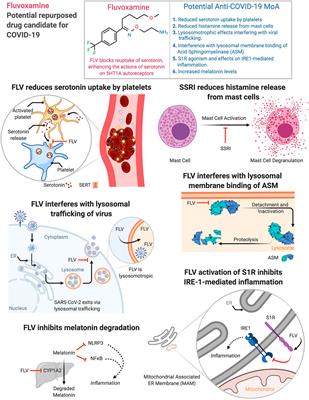
Why would an SSRI help with a viral infection?
Because you become depressed when you find out you have COVID.

Why would an SSRI help with a viral infection?
Because you become depressed when you find out you have COVID.
Why would an SSRI help with a viral infection?
 www.frontiersin.org
www.frontiersin.org
They’re good people trying to help at risk folks. Just seems like wasted energy right now to me.Haha! Maybe they specialized in "social EM"
That is the million dollar question. Why all this drug repurposing stuff? I could be wrong about this, but I think the root of it is the anti-vaccine movement. There are an enormous number of doctors producing shoddy research, rolling the dice with non-randomized, non-placebo controlled studies that get random, seemingly promising results. Many of these anti-vaccine people want the government and drug companies to focus on therapeutics, so that nobody would tell them that they needed to get vaccinated. The naturopathic type physicians at Home | America's Frontline Doctors and Home - FLCCC | Front Line COVID-19 Critical Care Alliance are putting out a massive amount of disinformation which is heavily influencing crunchy hippy type people, anti-vaccine, and anti-government folks, who bristle at vaccine mandates. For example, Robert Malone is a strange character who is employed by a private company to head up research, hoping to repurpose medications to be used against COVID and other diseases. They use in vitro methodology among other things. This guy, Robert Malone gave an interview on Joe Rogan, where he claimed to be using computer modeling to find drugs that would bind to various parts of a virus to inactivate it. We know that in vitro has no bearing often on clinical medicine. I would imagine that computer modeling would be way worse.Why would an SSRI help with a viral infection?
RM: once before I was infected at the end of February because I was attending a MIT conference on drug discovery and artificial intelligence so this is pre-lockdown February 20. but it goes back further than that um there's a CIA agent that I've co-published with in the past named Michael Callahan he was in Wuhan in the fourth quarter of 2019 he called me from Wuhan on January 4th I was currently managing a team that was focusing on drug discovery for organophosphate poisoning ergo nerve agents for DTRA, defense threat reduction agency, involving high-performing computing and biorobot screening um high-end stuff and he told me Robert you got to get your team spun up because we got a problem with this new virus I worked with him through prior outbreaks and so it was then that I turned my attention to this started modeling um a key protein a protease inhibitor of this virus when the sequence was released on January 11th as the Wuhan seafood market virus and I've been pretty much going non-stop ever since. I was self-treating myself after I got infected with agents that we'd identified through the computer modeling.
JR: so February of 2020 you get infected and how bad is your case
RM: bad I thought I was going to die you got to remember I was up up up on all the latest information from china and everywhere else I knew all about this virus I knew you know I I've been watching the videos of people dropping in the street my lungs were burning until I took famotidine and that relieved that
JR: and what is famotidine?
RM: it's otherwise known as pepcid so just to on this tangent since I've said it um I've got some good news to announce um first time here uh today we believe we should have the first patient enrolled in our clinical trials of the combination of monitoring and celecoxib for treatingSARS-CoV-2. This is trials being run by the company lidos which is one of my clients that I've helped design that's based on my discoveries they're funded by a defense threat reduction agency so this is another drug combination now I work with all these folks like Peter and Pierre um that I know you know
JR: Peter Mccullough, Pierre Cory
RM: but I haven't pushed this drug combination I just felt it was inappropriate until we got the trials running but they're now open and we've passed through the FDA screening process by the way we tried to get we had data showing that adding ivermectin further improve the combination but the FDA created such enormous roadblocks to us doing an ivermectin arm that we had to drop it and by we what I'm saying is the FDA created so much grief that the DOD decided it the juice wasn't worth the squeeze and they just dropped that arm
JR: why do you think that is what do you think is going on with the pushback on ivermectin
RM: So it's not just ivermectin, its hydroxychloroquine and just to put a marker on that there are good modeling studies that probably half a million excess deaths have happened in the United States through the intentional blockade of early treatment by the U.S. government that is familiar
JR: half a million
RM: half a million that is a well-documented number okay and it's the combination of hydroxychloroquine and ivermectin now when you ask me why you're asking me to get into somebody's head what I can say as a scientist is what I observe um the behaviors, the actions, the correspondence, these bizarre things like uh you know don't you know it's a horse drug y'all right which is amazingly pejorative I live in virginia okay I can tell you the people around me I live in a rural county and I raise horses um that was deeply offensive um to use that language in that way um but there's clearly been an intentional push and Zeb Zelenko who's a buddy the guy that came out with the original protocol zlanco protocol and was the one by the way that wrote the letter to um to trump advocating for hydroxychloroquine okay kind of important to put that together he's put together a great little video clip in which he clearly documents the conspiracy between Janet Woodcock and Rick Bright to make it so that physicians could not administer hydroxychloroquine outside of the hospital
JR: and who is Janet Woodcock and who's Rick Bright
RM: rick bright was the head of BARDA the biomedical advanced research director which is thegroup that for instance funded the JNJ vaccine and operational warp speed etc so they're thebig-ticket funder in health and human service of biodefense products
What is at the root of drug repurposing, like most things, is money.That is the million dollar question. Why all this drug repurposing stuff? I could be wrong about this, but I think the root of it is the anti-vaccine movement. There are an enormous number of doctors producing shoddy research, rolling the dice with non-randomized, non-placebo controlled studies that get random, seemingly promising results. Many of these anti-vaccine people want the government and drug companies to focus on therapeutics, so that nobody would tell them that they needed to get vaccinated. The naturopathic type physicians at Home | America's Frontline Doctors and Home - FLCCC | Front Line COVID-19 Critical Care Alliance are putting out a massive amount of disinformation which is heavily influencing crunchy hippy type people, anti-vaccine, and anti-government folks, who bristle at vaccine mandates. For example, Robert Malone is a strange character who is employed by a private company to head up research, hoping to repurpose medications to be used against COVID and other diseases. They use in vitro methodology among other things. This guy, Robert Malone gave an interview on Joe Rogan, where he claimed to be using computer modeling to find drugs that would bind to various parts of a virus to inactivate it. We know that in vitro has no bearing often on clinical medicine. I would imagine that computer modeling would be way worse.
That is the million dollar question. Why all this drug repurposing stuff? I could be wrong about this, but I think the root of it is the anti-vaccine movement. There are an enormous number of doctors producing shoddy research, rolling the dice with non-randomized, non-placebo controlled studies that get random, seemingly promising results. Many of these anti-vaccine people want the government and drug companies to focus on therapeutics, so that nobody would tell them that they needed to get vaccinated. The naturopathic type physicians at Home | America's Frontline Doctors and Home - FLCCC | Front Line COVID-19 Critical Care Alliance are putting out a massive amount of disinformation which is heavily influencing crunchy hippy type people, anti-vaccine, and anti-government folks, who bristle at vaccine mandates. For example, Robert Malone is a strange character who is employed by a private company to head up research, hoping to repurpose medications to be used against COVID and other diseases. They use in vitro methodology among other things. This guy, Robert Malone gave an interview on Joe Rogan, where he claimed to be using computer modeling to find drugs that would bind to various parts of a virus to inactivate it. We know that in vitro has no bearing often on clinical medicine. I would imagine that computer modeling would be way worse.
Maybe it's an effect on platelet function. We know COVID can cause hypercoagulability. SSRI's can inhibit platelet function (platelets need serotonin to fully function), so maybe they decrease coagulopathy?Why would an SSRI help with a viral infection?
I mean we still have the RECOVERY Trial that has been consistently doing much of the work since 2020. If we stick to that trial and ignore crappy prospective studies elsewhere, that should be more than plentyFor the reputable people looking at drug repurposing it’s because it’s lower clearance to wide use because safety trials are largely done.
It’s really hard to do a high quality trial during a pandemic, but there’s no excuse for the crap some people have put out. What I’d like to see is that we learn from this and have some standardized designs ready to go if we’re ever in this situation again, and some reputable centers and researchers/teams designated to do certain studies so it’s not some international free for all with some efforts being duplicated and some important stuff not being done right away.
Today I got my first patient that was prescribed ivermectin by a legit physician. Like 20 pill of ivermectin a day for 2 weeks, the FLCCC protocol.
Out of morbid curiosity I did check out their website what the cool kids are doing these days
The prevention regimen seems to be ivermetin two times a week (you can substitute black cumin seed), antiseptic mouthwash gargle 2x daily, vitamin cocktail of D3, C, Quercetin, Zinc, Melatonin,
Early treatment protocol seems to bump ivermectin to daily + nitazoxanide, Mouthwash is 3x daily now + iodine nasal spray. Add aspirin 325 to the vitamin cocktail. Second line agents here includes double anti-androgen therapy (spironolactone + dutasteride), fluvoxamine (but you can substite fluoxetine), and MAB goes here too.
For me, it seems to be easier to just get the vaccine then this pretty complicated (and obviously very effective) protocols. There's also a Long Hauler protocol.
Aspirin is probably doing all the work here...Today I got my first patient that was prescribed ivermectin by a legit physician. Like 20 pill of ivermectin a day for 2 weeks, the FLCCC protocol.
Out of morbid curiosity I did check out their website what the cool kids are doing these days
The prevention regimen seems to be ivermetin two times a week (you can substitute black cumin seed), antiseptic mouthwash gargle 2x daily, vitamin cocktail of D3, C, Quercetin, Zinc, Melatonin,
Early treatment protocol seems to bump ivermectin to daily + nitazoxanide, Mouthwash is 3x daily now + iodine nasal spray. Add aspirin 325 to the vitamin cocktail. Second line agents here includes double anti-androgen therapy (spironolactone + dutasteride), fluvoxamine (but you can substite fluoxetine), and MAB goes here too.
For me, it seems to be easier to just get the vaccine then this pretty complicated (and obviously very effective) protocols. There's also a Long Hauler protocol.
Today I got my first patient that was prescribed ivermectin by a legit physician. Like 20 pill of ivermectin a day for 2 weeks, the FLCCC protocol.
Out of morbid curiosity I did check out their website what the cool kids are doing these days
The prevention regimen seems to be ivermetin two times a week (you can substitute black cumin seed), antiseptic mouthwash gargle 2x daily, vitamin cocktail of D3, C, Quercetin, Zinc, Melatonin,
Early treatment protocol seems to bump ivermectin to daily + nitazoxanide, Mouthwash is 3x daily now + iodine nasal spray. Add aspirin 325 to the vitamin cocktail. Second line agents here includes double anti-androgen therapy (spironolactone + dutasteride), fluvoxamine (but you can substite fluoxetine), and MAB goes here too.
For me, it seems to be easier to just get the vaccine then this pretty complicated (and obviously very effective) protocols. There's also a Long Hauler protocol.
The Front Line Covid-19 Critical Care Alliance, the group that has been suing hospitals to administer ivermectin. Their webpage and all their various "protocols" Home - FLCCC | Front Line COVID-19 Critical Care AllianceFLCCC?

I still always thinks its weird to be taking 5-8 methotrexate pills/week for RA even though I know better.The Front Line Covid-19 Critical Care Alliance, the group that has been suing hospitals to administer ivermectin. Their webpage and all their various "protocols" Home - FLCCC | Front Line COVID-19 Critical Care Alliance
Although I will note that this family medicine doctor who wrote this prescription didn't seem to be following the "FLCCC protocol" she cited. As she wrote for 14 days of ivemerctin overdose instead of the recommended "5 days". I don't think I have ever written for ivermectin and have written for nitazoxanide maybe one time (for HIV cryptosporidium diarrhea). But I have a philosophy. If I am thinking about writing for 12 tablets of ANYTHING as a single dose (let along for 2 weeks), maybe don't write that prescription.
Protip to patients: if your doctor writes you to take 12 tablets of anything, he may be trying to murder you.
Also, the indication on the prescription seems to be "cough", so I'm not sure any pharmacy would actually fill that out.
A very sizable portion, if not a majority, of medications dispensed every day in the United States are for "off-label" use.Warning for those of you prescribing drugs for "off-label" use. Not a bad practice per se . Just better make sure your patients are signing consents specifically stating the medication is off-label, non-fda approved for the condition and you LIST all the side effects. Any bad outcome otherwise and you're on the hook.
A very sizable portion, if not a majority, of medications dispensed every day in the United States are for "off-label" use.
As just one example, gabapentin is only approved for postherpetic neuralgia and as an adjunctive therapy in the treatment of a subset of partial onset seizures. However, I would be shocked if that amounted to even 5% of the amount actually prescribed.
No one is getting specialized consent for "off label" use.
You do that for all off-label meds?I do. I have a small concierge practice and I have a specialized consent forms for off label medications I frequently write for ( just three medications but they are sensitive medications).
Does not matter how many doctors are doing it. If you're prescribing a medication for a non-FDA approved condition and not consenting your patients for it including side effects, you open yourself to liability if there's a bad outcome. It's just good medicine.
.There was a local doctor here in town that was treating patients with off-label peptides. One of them had an MI and the wife sued. "Didn't tell me this can cause MI". Doctor settled.
You do that for all off-label meds?
I haven't heard of anyone doing this before. Would you mind sharing the meds and indication you do this for?If they have the potential for badness or are sensitive drugs, then yes, I'll have them sign the consent and initial next to each side effect. Low risk medication? Probably just a verbal consent and document it.
Do you (or would you) use propranolol for thyroid storm or hepatic portal hypertension?I do. I have a small concierge practice and I have a specialized consent forms for off label medications I frequently write for ( just three medications but they are sensitive medications).
Does not matter how many doctors are doing it. If you're prescribing a medication for a non-FDA approved condition and not consenting your patients for it including side effects, you open yourself to liability if there's a bad outcome. It's just good medicine.
.There was a local doctor here in town that was treating patients with off-label peptides. One of them had an MI and the wife sued. "Didn't tell me this can cause MI". Doctor settled.
Add me to the "CTA every hypoxic covid patient" regardless of the d-dimer. I can't tell you how many PEs I've found. Perhaps it's excessive, but at least our hospitalists are great at accepting the patient prior to the CTA result being back, to which they follow up on results.
With the current medicolegal environment, and without evidence-based "guidelines" on how to clinically rule out PEs in hypoxic COVID patients, I personally think an EP is taking on a ton of risk by not approaching it this way.
.There was a local doctor here in town that was treating patients with off-label peptides. One of them had an MI and the wife sued. "Didn't tell me this can cause MI". Doctor settled.
If they have the potential for badness or are sensitive drugs, then yes, I'll have them sign the consent and initial next to each side effect. Low risk medication? Probably just a verbal consent and document it.
There is a very good chance that you are increasing your malpractice risk, not reducing it.I do. I have a small concierge practice and I have a specialized consent forms for off label medications I frequently write for ( just three medications but they are sensitive medications).
Does not matter how many doctors are doing it. If you're prescribing a medication for a non-FDA approved condition and not consenting your patients for it including side effects, you open yourself to liability if there's a bad outcome. It's just good medicine.
.There was a local doctor here in town that was treating patients with off-label peptides. One of them had an MI and the wife sued. "Didn't tell me this can cause MI". Doctor settled.
That seems like a leap. There's quite a gulf between a common off label use for a civilian who fills the Rx and takes it at home vs surreptitiously giving a rogue med to people who have been stripped of their freedom.Found this gem:
"Detainees at an Arkansas jail who had Covid-19 were unknowingly treated by the detention center’s doctor with ivermectin, a drug that health officials have continually said is dangerous and should not be used to treat or prevent a coronavirus infection, according to a federal lawsuit filed by the American Civil Liberties Union on behalf of four detainees."
"The lawsuit says the men “ingested incredibly high doses” of the drug while sick with Covid, causing some to experience diarrhea, bloody stools, stomach cramps and issues with their vision."
"She added that after the American Civil Liberties Union began to raise questions about the practice last year, the jail tried to get inmates to sign forms saying that they retroactively consented to the treatments."
Detainees Sue Arkansas Jail That Gave Them Ivermectin to Treat Covid
For months, the jail’s doctor has promoted the drug, which health experts say should not be used to treat or prevent Covid-19.www.nytimes.com
Warning for those of you prescribing drugs for "off-label" use. Not a bad practice per se . Just better make sure your patients are signing consents specifically stating the medication is off-label, non-fda approved for the condition and you LIST all the side effects. Any bad outcome otherwise and you're on the hook.
Do you (or would you) use propranolol for thyroid storm or hepatic portal hypertension?
Do you use colchicine for pericarditis?
Do you use high dose albuterol for hyperkalemia?
Do you use erythromycin to improve gastric emptying (for example, prior to EGDs)?
Do you infuse albumin at 1.5 mg/Kg within 6 hours of DX and 1 mg/Kg at day 3 for SBP patients with renal failure? (AASLD class 2a, level B recommendation)
Do you use 4 factor PCC (KCentra) for severe bleeding with DOACs?
Do you use TXA for severe post partum bleeding (WOMAN trial), non-neurological major trauma (CRASH-2), neurological trauma (CRASH-3), or based on TEG/ROTEM results?
So you're prepared to discuss the risks of off label uses for these medications... or not use them at all then?
Just because it isn't in the label doesn't mean it also can't be a part of the standard of care.
Maybe, maybe not. One medmal attorney told me " you can never have enough consent".There is a very good chance that you are increasing your malpractice risk, not reducing it.
The question is whether all the extra work properly shields you in a worst case scenario.
"If there is a bad outcome, a lawyer will find blame whether it's there or not."
We are finding lots of PEs on admitted COVID. My practice is adjusting to CTA anyone with ddimer over age adjusted level - which unfortunately is a lot. The hospitalist accepts them with the CTA pending.
This might be the greatest post on SDN yet. I'm just sad that 3% of patients don't get the Shpeel on vaccination.Regeneron (casirivimab and imdevimab) and Eli Lilly (bamlanivimab) are not effective against Omicron. And right now I'm assuming everybody has Omicron because it's penetrance is like 85-90% last I checked.
There is very little treatment, if any, that I offer. My workflow:
Code:if (symptoms sound like COVID) { if (SpO2 > 90% RA or if borderline, exertional SpO2 > 90% RA) { // there is basically nothing I do for definitive treatment in this group, e.g. no MABs // 99 of 100 people in this group get discharged, and the one that doesn't must fight to be admitted - reciteShpeel("there is nothing to do. Hope you don't get sick. You are putting up the good fight. COVID is at least 10x worse than flu. You are going to do fine. Don't see Grandma or Grandpa over the next week. No, you can't have ivermectin."); if (random number between 1-100 is > 3) { - reciteShpeel("Please consider getting vaccinated after you recover from this."); } // however there are special subpopulations that I might do something: if (vitals are out of whack for routine COVID infection) { - they still prob. have COVID, but I consider PE, bacterial PNA, etc. workup accordingly } else if (age > 70ish) { - I usually send CXR and basic labs, but mostly for show. People can't fathom - going to the doctor and doing nothing. I still don't treat though. } else if (super demented or bedbound w/ poor protoplasm) { - send basic labs and CXR - reciteShpeel("Oh your demented, mute mother is dehydrated!"); - give 1L LR - give ofirmev } - send COVID Rapig Ag test - +/- supportive care meds (Toradol, tylenol, zofran, promethazine, etc). - discharge immediately, callback if (+), do not callback if (-). } else { // here SpO2 < 90% // you get admitted - BMP, Mg, CBC, LFTs, Lactate, BCx x2, Ferritin, C-RP - CXR - COVID PCR test - supportive care meds if needed - ADMIT } }
I missed it with the first time it was posted, but I love the programming part!This might be the greatest post on SDN yet. I'm just sad that 3% of patients don't get the Shpeel on vaccination.
I'd be interested to know what the approximate yield on this practice is. I don't think it's necessarily wrong, as long as radiology can accommodate it. Especially if the hospitalist is accepting the patient with the scan pending. (From their perspective, I can see why they would want everyone scanned off the bat. It can be a pita to get people scanned from the floor and it can really help differentiate things if/when the patient decompensates, esp in a situation when you're covering too many patients to be able to reevaluate them frequently.)We are finding lots of PEs on admitted COVID. My practice is adjusting to CTA anyone with ddimer over age adjusted level - which unfortunately is a lot. The hospitalist accepts them with the CTA pending.
This has been my experience as well. Very few hypoxic covid patients have ended up having PE for me. I generally don't pursue CTA unless they are stepdown level to begin with or clinically worsening on steroids.I would say there is definately confirmation bias with covid-19 and PE. When we looked at our local PE prevalence pattern even in admitted patients, it is magnitude lower than what some of the papers are describing. Routine scanning of all patient in the ED is a complete waste of time.
I am overseeing our PE discharge protocol and pull all PE diagnosis made every 30 days (for both admission and discharge). I also check every CTA PE protocol ordered. Out of my random sampling of the CTA PE orders, the positivity rate is no more with Covid patients than it is with non-Covid patients. I have been checking Covid status (when known) for all charts I've reviewed. The vast majority of Covid patients that are hypoxemic with non-impressive chest x-rays usually have multifocal pneumonia as the cause of their hypoxemia.I would say there is definately confirmation bias with covid-19 and PE. When we looked at our local PE prevalence pattern even in admitted patients, it is magnitude lower than what some of the papers are describing. Routine scanning of all patient in the ED is a complete waste of time.
Every bit of the literature reports what you have seen, unless you think they have a PE don’t scan them. +\- COVIDI am overseeing our PE discharge protocol and pull all PE diagnosis made every 30 days (for both admission and discharge). I also check every CTA PE protocol ordered. Out of my random sampling of the CTA PE orders, the positivity rate is no more with Covid patients than it is with non-Covid patients. I have been checking Covid status (when known) for all charts I've reviewed. The vast majority of Covid patients that are hypoxemic with non-impressive chest x-rays usually have multifocal pneumonia as the cause of their hypoxemia.
I am overseeing our PE discharge protocol and pull all PE diagnosis made every 30 days (for both admission and discharge). I also check every CTA PE protocol ordered. Out of my random sampling of the CTA PE orders, the positivity rate is no more with Covid patients than it is with non-Covid patients. I have been checking Covid status (when known) for all charts I've reviewed. The vast majority of Covid patients that are hypoxemic with non-impressive chest x-rays usually have multifocal pneumonia as the cause of their hypoxemia.
I randomly sample patients, so not statistically significant. Somewhere around 10% with a positive D-dimer and less than that without.What percentage of all PE studies ordered result in + PE?
I just can’t wrap my mind around fluvoxamine. I think I wouldn’t believe evidence, even if it were presented to me about it. I feel the same way about Ivermectin. At least Hydroxychloroquine had some anti-inflammatory effects that made some physiological sense. I think we sometimes believe certain studies and adopt certain practices because they make us feel more wise than our peers. “I am practicing cutting edge medicine!” But, when we see somebody else practice on the fringe, we think “what in the hell is that wack job doing?”In Medicine, it's better to be wrong and in the herd, than correct and apart from the herd.
In Medicine, you are punished for thinking and acting outside the box. This is not art, music, entrepreneurship or creative writing, where those things new, risky, edgy and against the grain are prized. If you act outside the accepted norm, you're more likely to be punished, than not. It doesn't matter if you turn out to be right, in the end. You'll be punished in the meantime and without apology. It's even codified into law: "THE. STANDARD. OF. CARE."
What if the standard of care turns out to be wrong and you were right? Nothing, other than you'll be punished for "violating the standard" when it was standard. "Standard of care" in medicine turns out to be wrong, and changes, so often, you could almost consider it being wrong and eventually changing, the norm. You'll never receive and apology letter after the fact saying, "Sorry, all of Medicine was wrong. But you were right. Good job." The last thing you want to be in Medicine is the guy that's right, before everyone else is. The only thing nerds hate more than someone that thinks they're smarter than them, is someone that is smarter and not afraid to show it.
I randomly sample patients, so not statistically significant. Somewhere around 10% with a positive D-dimer and less than that without.
I think without a d-dimer it's like 5% are positive. I'll have to look at the numbers.One time at work I was killing time with nothing to do…and I pulled up the last 50 CT PE studies ordered by ER physicians. Knew nothing about the cases, whether a ddimer was even run, it’s result, etc. 49 / 50 were negative.
I think without a d-dimer it's like 5% are positive. I'll have to look at the numbers.