- Joined
- Jan 13, 2010
- Messages
- 1,671
- Reaction score
- 480
7 years ago there were thousands more partnership jobs than there are today.
This is a major strawman. The original hypothesis said nothing about partnerships. It was about salary.

7 years ago there were thousands more partnership jobs than there are today.
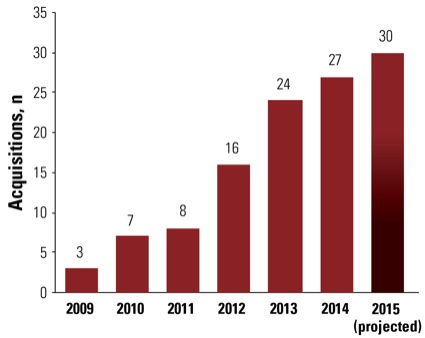
Take a look at this graph since 2009 and tell me things haven't changed significantly:
You've monkey-barred to a completely different assertion since your half-empty glass of future compensation has been proven woefully incorrect.
Most statistics about compensation say that anesthesiologists salary has not declined, let alone the drastic amount you stated 7 years ago.
To play devil's advocate, you think private equity groups with smart people would be investing in a dying specialty? There are many ways to look at this.
The specialty is dying BECAUSE of private equity.
It's not scientific, but in the two years I've been looking for jobs, compensation has decreased and workload has increased. The ceiling or potential income that one could earn in anesthesiology is significantly less now than it was in 2009. Income isn't everything when you talk about a "great gig," but working your butt off for 65 hours a week, taking in house call, getting 4 weeks vacation and making 350k is becoming the reality at a lot of these employed positions for private equity groups. I'm not so sure that's a great gig, no matter how much you like anesthesia.
You think if fam med truly paid 240k with no calls or wknd and 45hr work week that the job market wouldnt be flooded in another 5 or 10yrs, med studemt will be all over that opportunity like white on rice...if there is any field in medicine that is primed for complete annihilation by midlevel and over supply of providers its family med and psych. And those figures you quote is very regional, most fam med are not msking 240k base with no calls wknds...
I have to respectfully disagree on this one.
I think primary care has tremendous growth potential for physicians, despite all of the concern about midlevel encroachment and the historically low pay (relative to specialists). I think any field that sees a disproportionately high number of "undifferentiated" patients--i.e., patients with no prior diagnosis for their presenting symptoms and signs--is ideally suited for physicians, especially if the goal is to maintain high quality care/good patient outcomes and minimize overall cost in the healthcare system as a whole.
In a primary care setting, these goals become somewhat mutually exclusive if systems rely too heavily on nurse practitioners. A nurse practitioner fresh out of training cannot possibly know as much as an internist or family medicine doctor right out of residency. Nurse practitioners have a bachelor's degree in nursing + 1-2 years of postgraduate training. Internists or family med doctors have a bachelor's degree + 4 years of med school + 3 years of residency. I'm not a mathematician, but I'm pretty sure that 6 does not equal 11. The MCAT/USMLE Step 1/USMLE Step II CK/USMLE Step II CS/USMLE Step III/Specialty board examination collectively do not equal the NCLEX and GRE. These differences in training and credentialing matter in undifferentiated patients. You need the larger theoretical knowledge base and clinical experience to work up these patients and do it in a way that minimizes cost without compromising quality. Could a nurse practitioner work these patients up? Sure. But it will be at a higher cost due to unnecessary tests and consultations.
Now, when artificial intelligence works its way into clinical medicine, the playing field may become truly equal between physicians and midlevel providers in the areas of cost and quality. But we're not there yet. Until technology can make up for the relative deficiencies in theoretical knowledge and clinical exposure, physicians will remain the best suited clinicians to evaluate undifferentiated patients, especially complex cases.
The other great thing about primary care is that it's in a fantastic position to operate outside of insurance. Income for these direct care physicians is excellent, in many cases on par or exceeding specialist income. For many specialists (myself included), it would be nearly impossible to not take insurance. It's not like I can start implanting spinal cord stimulators or injecting cement into the spine on a cash basis. The average patient can't possibly afford the cost of the stimulator hardware or tools required for vertebral augmentation. The situation is even worse for surgical subspecialists who routinely implant hardware or rely heavily on sophisticated intraoperative technology. I can't imagine cardiac surgeons as a group pulling out of insurance. Only the filthy rich can afford to pay cash for heart surgery.
I'm happy for the primary care docs enjoying a boost to their field in terms of income, job opportunities, and autonomy. It's long overdue. The specialty has been s%&* on for too long. They deserve to be paid well.
That is anecdotal. I went into private practice 2 years ago and every one of my residency colleagues I keep in touch with found very good jobs they are happy with. Only one has switched from his original gig. And again, statistics do not back up the original assertion. That's all there really is to it.
This place is such a far deviation from the real world that I feel a need to offer the other side of the story. It's like a hangout for embittered practitioners. Which is fine. Y'all just need to know that the world may not exist to others as you see it.
And it's easy to say something and not be right.
That is anecdotal. I went into private practice 2 years ago and every one of my residency colleagues I keep in touch with found very good jobs they are happy with. Only one has switched from his original gig. And again, statistics do not back up the original assertion. That's all there really is to it.
This place is such a far deviation from the real world that I feel a need to offer the other side of the story. It's like a hangout for embittered practitioners. Which is fine. Y'all just need to know that the world may not exist to others as you see it.
This is a major strawman. The original hypothesis said nothing about partnerships. It was about salary.
I'm guessing you are in a less populated area of the country and are thus a standard deviation or two away from the mean. Your evidence to the contrary is purely anecdotal as well based on your friends' experiences post residency. Again, the vast majority of jobs exist within these highly populated and highly desirable areas. Desirable area is obviously a relative term, but some people value proximity to family and these private equity firms know that and take advantage of it.
I can't believe you posted that statement. SALARY is directly linked to PARTNERSHIP as that is where the real money is earned.
Let's review the facts:
1. Your statements are anecdotal. I have provided evidence which shows a major shift in the paradigm of anesthesia employment which results in lower salaries.
2. That paradigm shift is accelerating (again the evidence is clear)
3. Salaries for employee positions are much lower than Partnership at private groups
4. Your "statistics' are anything but factual. Your claims are not backed up by the jobs available to the majority of Residents without connections. (see www.gaswork.com)
5. The are pockets of private groups throughout the USA with the most successful ones in the Midwest.
6. You are entitled to your own opinion but not your own facts. The job market is NOT a good one in 2016 and much worse than 2009.
7. The top 20% of groups NOT receiving a subsidy are doing quite well. The schism between the top quartile and bottom quartile has never been wider.
A 4th year Med Student is probably looking at an employee type position post residency. Anyone who posts otherwise is creating a false sense of optimism for the majority who enter this specialty. Like ER/EM Anesthesiology is slowly moving towards a salary or hourly rate of employment with the contract held by the hospital or management company.
The exact timing of when a bubble will burst is difficult. But, the evidence clearly shows that hundreds of groups have sold out or folded since 2009. This means income went down in those hospitals for many anesthesiologists.
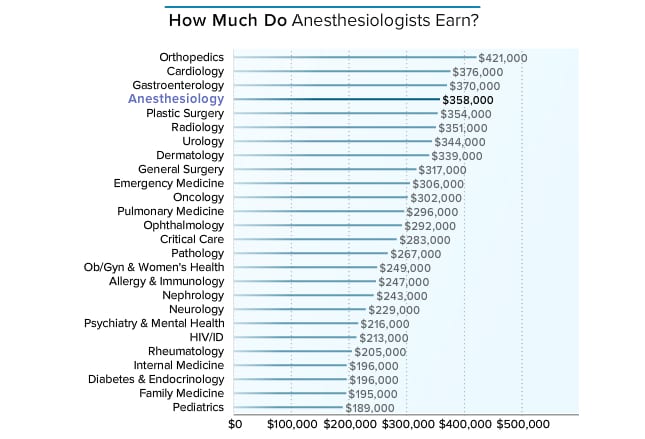
The "N" in these surveys is low and I think you need to compare the survey number with the actual number of Anesthesiologists in the work place. Do you think that surveying 4 percent of Anesthesiologists in an non random manner predicts salary? The trend is downward and has been that way the past few years. That said, about 1/4 of PP attendings are earning record income while the bottom 1/4 scrounges for low paid work. There is a glut in the market place which forces salaries downward. This fact is best shown in the trending of academic salaries. If things are so rosy out there why does academic pay keep declining in your chart? Is it because there is a glut of labor for the Chairs to squeeze extra hard?
Employed anesthesiologists make $318,000, which is less than their self-employed counterparts ($410,000).
Do you think that surveying 4 percent of Anesthesiologists in an non random manner predicts salary? The trend is downward and has been that way the past few years.
http://www.medscape.com/features/slideshow/compensation/2015/anesthesiology#page=3
Dude, you made a prediction that was woefully, 100%, no questions need to be asked, absolutely INCORRECT. What- things change over time? Is that what you are saying? Wow. Crazy! If you review the link, you'll see in fact anesthesia compensation is very good and actually on the rise.
Compensation is not on the rise. There is a skewing of salaries towards the Median of $357,000. More and more private practice gigs are going the way of the dinosaur and as that occurs the Median becomes a larger number in that survey. In the past, many like myself would never disclose our true salary because the hospital would cut our stipend. It was in our best interest to keep any posted number LOW.
I have made my points on this subject quite clear. I will defer to the reader to decide which argument makes the most sense.
Yes the one that makes the most sense is backed up by data.
" Furthermore, the MGMA Report indicates that between 2008 and 2012, anesthesiologist compensation increased in every year but 2010."
Not according to the Medscape compensation report I just posted. You were wrong. Just admit it. I know it is hard for many of us doctors, and no one is saying you could be right in the future, but geezus man. Give me a break.
Data that is a non random survey of 6% of Anesthesiologists. I can tell you the income of many specialties on that survey is flat out wrong.
Salary is only a piece of the picture. Salary may be the same or slightly better, but you are working ALOT more for it. Making 350 and working 40 hours a week with 8 weeks of vacation is ALOT different than making 350 and working 65 hours a week with 4 weeks of vacation. The latter scenario is the much more common job that new anesthesiologists will be getting. That's what these private equity companies are paying for now. Sure, salary is the same, but that is not the full story. You also don't have the psychological satisfaction of earning more as you work more. Nowadays if you work more, the guy in the suit who owns you earns more.
Anesthesia as a speciality is fun to practice, but the business end of it is just awful right now. I do agree with earlier postings that primary care is on the upswing.
This is a major strawman. The original hypothesis said nothing about partnerships. It was about salary.
I'm not saying the original hypothesis was perfectly true. I'm saying there's truth there if you look at the subgroup of more recent residency grads. What was the income of an anesthesiologist with 5 years experience in private practice 7 years ago and what is it today? I bet you for many, many practices it is 20-25% lower because people who would have made partner by now 7 years ago but are permanently kept as salaried employees these days. Sure people who got in before the downfall of private practice anesthesia/takeover by AMCs are mostly still making lots of money, but this specialty has declined significantly in the last several years and is declining more and more each year. Hopefully it will level out and some competition between AMCs will keep incomes near current levels, but the good old days are over and are never coming back.
Data that is a non random survey of 6% of Anesthesiologists. I can tell you the income of many specialties on that survey is flat out wrong.
Once again, you're launching a straw man to try and compensate for your completely erratic prediction 7 years ago.
Perfectly true? It was 100% false!
You are 100% wrong. You really are. Take the rose-colored glasses off and enjoy the real world, my friend.
That's not ow I see it slim. Private Groups are being taken over or dismantled in larger numbers each year. This means salaries are falling for thousands of Anesthesiologists SUBSTANTIALLY each and every year as the AMC/Hospital cuts their pay and increases the work load. I have provided solid evidence that this is occurring at an accelerating pace since 2009. How you can't connect the dots that this means salaries are DECREASING at a rapid pace towards the median I can't understand.
Sorry. I like actual data. Not "I looked at gaswork" data.
For those reading, life is good in private practice and come on board if you enjoy the specialty.
What percentage of new grads do you think will end up in a real life, true private practice? Let's say for the med student reading this now who would be graduating in 4-5 years? Again, you can't use caveats saying well, it depends on the area of the county. I am talking about the country as a whole where the vast majority of the population and thus the vast majority of the jobs exists on the coasts.
Again, evaluating the quality of a career based on one data point of average salary really gives an incomplete picture of the story.
What percentage of new grads do you think will end up in a real life, true private practice? Let's say for the med student reading this now who would be graduating in 4-5 years? Again, you can't use caveats saying well, it depends on the area of the county. I am talking about the country as a whole where the vast majority of the population and thus the vast majority of the jobs exists on the coasts.
Again, evaluating the quality of a career based on one data point of average salary really gives an incomplete picture of the story.
And just having salary data published by the MGMA is only a very very small part of the story.
So are anecdotal stories. In fact, I would say they aren't even part of the story at all. They are too rooted in bias.
If things are so good out there why have 160 groups sold to management companies since 2009?
It really makes no sense to me how you can post a graph showing average salary and say "see, things are getting better, not worse." Salary is a pretty meaningless number without evaluating the job environment as a whole. Any AMC can come in and buy your practice and keep the salary the same or even increase it....but they are cutting your vacation time in half and making you work double the amount of average weekly hours. That's the point. Your salary is the same, but how you are being valued is getting worse.
If things are so good out there why have 160 groups sold to management companies since 2009?
I can think of two explanations, off the top of my head, that may or may not be true:
1) FUD
2) Venture capitalists don't always make good decisions; extraction of short-term cash from something doesn't mean that long-term prospects are either good or bad
Maybe 160 groups scammed some doomed management companies out of a bunch of cash. What did they really sell? What's a group's contract really worth? History with the hospital? Good will?
Every time I hear a group has sold out, I think, hmmm, I wonder if in 3 or 5 years the management company might be run out of town on a rail, and those same doctors might go back to a system that's sick of dealing with a faceless corporation that gave them a bunch of retread locums problem children.
Probably not. But N sellouts isn't proof that AMCs will rule the world.
They might. I would not be completely surprised if when I leave my current "employed" position in a few years, that my best option will be another employed position. But the fact that the last few years I've watched a bunch of superpartners cash out (generally at the expense of their juniors) doesn't necessarily mean much. All it proves is that a relatively small number of people made the best business decision they thought they could make at that moment in time.
160 groups is not a small number especially with a trend that is accelerating. In addition, many hospitals are taking anesthesia "in-house" to by-pass the management companies altogether. The groups that will be left are those large enough to deal with all the issues and documentation required by the Federal govt. This means even more mergers or acquisitions in the future.
Whether the group has sold out or just been eliminated by the hospital the trend is quite clear that small private groups are on the endangered species list. Those with business sense are seeing the trend and looking into merging with other groups. The best way to survive going forward is to get bigger as it leads to higher reimbursement and the ability to cope with ever increasing Federal regulations.
The average Resident graduating in 2016 is faced with a tougher road ahead. There are opportunities out there in less than perfect locations and those are where one should go to make some money before everyone becomes an employee of some sort. Make hay while the sun shines.
With declining partnership opportunities (FACT) comes declining income no matter what any survey seems to indicate. I think Median wages will stay in the $360K range but the benefits could be poor (like AMCs) and the workload quit heavy. I seriously doubt middle America will be shedding any tears over your "declining" $360K salary.
I bet the pace of groups selling decreases over the next several years. AMC are not a long term solution.
Reason blade and all the other AMC members on here push doom n gloom is so that your group sells. If your group sells blades stock value increases and his group might even see a bonus from your groups acquisition. Or if you still belong to a non public AMC your goal is to grow so that it goes public and then you get a nice bonus from your stock options. Sounds great for the profession.
Rubbish. I have no plans to remain with an AMC and don't own a single share of any of those stocks. I recommend working for a hospital or Academic center over an AMC. I hope all the AMCs go out of business and private practice returns to the market. This entire system we have in place makes no sense except to enrich the middleman at our expense.
Let's hope the AMCs all go out of business soon but things move slowly in medicine and insurance. Best of luck to those trying to make a good living doing Anesthesiology these days. The opportunities are still there just a lot fewer than in 2009. I still think a fellowship followed by the willingness to go where the good jobs are makes for the best financial plan.
Even with real median income down for 2016 vs 2009 due to employee positions, sale of private groups and hospital take-overs the median job still pays over $360K. I don't push "doom and Gloom" but rather try to state things as they are rather than as what people want them to be. Realism is what this thread is all about. I bet the average med student won't be discouraged from this field based on the fact that income is $360K in 2016 vs $450K in 2009. The loss of autonomy, ratios of 4-5:1, the rise of the solo CRNA, etc are all as important as the drop in salary.
Most Residents don't have a connection to find a job. Those that do should use it to secure a real private partnership track when possible. AMCs should be reserved for those people who can't find jobs anywhere else or must live in a certain location.
AMCs remind me of the Dot com era of 1998-2000. We all know how that ended. Still, some people got very rich selling crappy companies for hundreds of millions of dollars.
I must have misunderstood one of your previous discussions. I was assuming you took a partial buyout (cash and stock) based on that discussion.