Well, it's not just we docs. Take cardiac - most of us on the anesthesiologist side will not only admit, but will argue, that any residency-trained anesthesiologist is absolutely capable of doing the great majority of cases involving CPB. It may take some extra effort to get the requisite TEE experience, but it's reasonable to expect a resident to get that training in initial residency, and to be able to hone it as an attending.
But what's happened?
NBE decreed (way back in 2009) that a 1-year fellowship dedicated to the perioperative care of cardiac surgical patients was needed to achieve board certification in TEE. The practice pathway to certification was slammed shut on July 1st, 2009. Oh, they'll still take your money and let you take the exam, but now you have to be content with the Testamur title.
Since about that time, more and more hospitals have gradually changed their policies to make it difficult or impossible to credential non-fellowship trained anesthesiologists to do hearts. So groups can't hire someone to do hearts if they don't have the fellowship. So anesthesiologists who want to do hearts, who aren't already entrenched into their current institution's heart program, need to do the fellowship.
My own hospital literally shut down its cardiac surgery program for a month because there was a gap between the loss of the last cardiac-credentialed anesthesiologist, and my arrival from fellowship. I'm a swell dude, but I'm not that special. Never mind that we've got a department of 30-something anesthesiologists, including some who did cardiac at other institutions before coming here. There's no reason at all that any one of them couldn't have stepped in and done the cases. Perhaps with a cardiologist stepping into the room to help with the TEE, but it could've been done. If not for the credentialing issue.
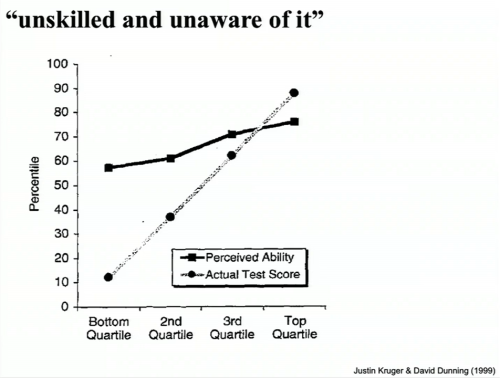
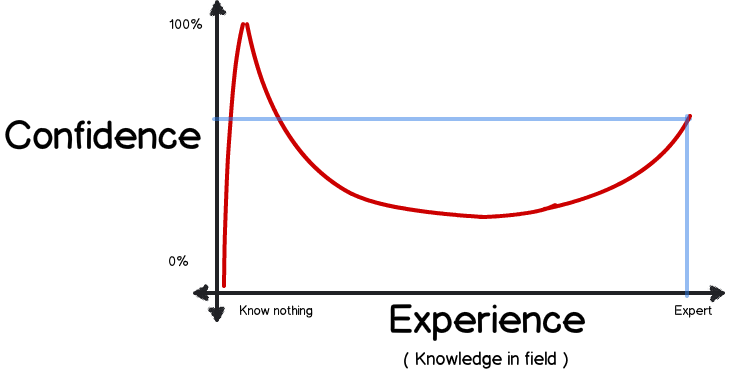
The only sense in which we docs keep upping the ante is our recognition that as the years go by medicine gets more complex, the care of a subset of complex patients benefits from physicians who've had additional subspecialty training. This is a good thing; this is a reflection of the fact that people in our profession are largely on the correct side of the Dunning-Kruger curve.