- Joined
- May 23, 2014
- Messages
- 86
- Reaction score
- 12
Ebola Update Thread
Officially Reported Statistics through January 25th, 2015
(Actual Number of Cases and Deaths is higher, possibly two times higher, than reported numbers).
Total Number of Officially Confirmed Cases: 22,057
Total Number of Officially Confirmed Deaths: 8,795
Total Number of Officially Confirmed Cases one month ago was 19,810
Liberia: Approximately 614 (8/11), 776 (8/18), 1049 (8/26), 1307 (8/31), 1492 (9/6), 1861 (9/10), 1924 (9/14), 2188 (9/17), 2186 (9/25), 2136 (10/1), 1681 (10/12), 2795 (10/24), 2695 (11/4), 2629 (11/11), 846 (12/14), 383 (12/24), 273 (1/25) new official cases in the past month
Sierra Leone: Approximately 424 (8/11), 465 (8/18), 493 (8/26), 642 (8/31), 644 (9/6), 779 (9/10), 863 (9/14), 905 (9/17), 1094 (9/25), 1221 (10/1), 1670 (10/12), 1996 (10/24), 2073 (11/4), 2334 (11/11), 2527 (12/14), 2337 (12/28), 1315 (1/25) new official cases in the past month
Guinea: Approximately 113 (8/11), 169 (8/18), 176 (8/26), 299 (8/31), 367 (9/6), 393 (9/10), 423 (9/14), 422 (9/17), 455 (9/25), 428 (10/1), 506 (10/12), 524 (10/24), 462 (11/4), 447 (11/11), 470 (12/14), 552 (12/28), 287 (1/25) new official cases in the past month
Total Reported Cases Liberia: 8,622 (3% of these cases reported in the past month).
Total Reported Cases Sierra Leone: 10,518 (13% of these cases reported in the past month).
Total Reported Cases Guinea: 2,917 (10% of these cases reported in the past month).
The trend over the past couple months with regards to total numbers of new official Ebola cases in West Africa seems to have leveled between 800 and 1200 cases per week, however it was recently reported that the total number of officially reported cases for the region has fallen to around just 100 per week. Nonetheless, there are probably a similar number of unreported cases (possibly a hundred or more a week) as some recognized cases do not have contacts with any other known Ebola cases.
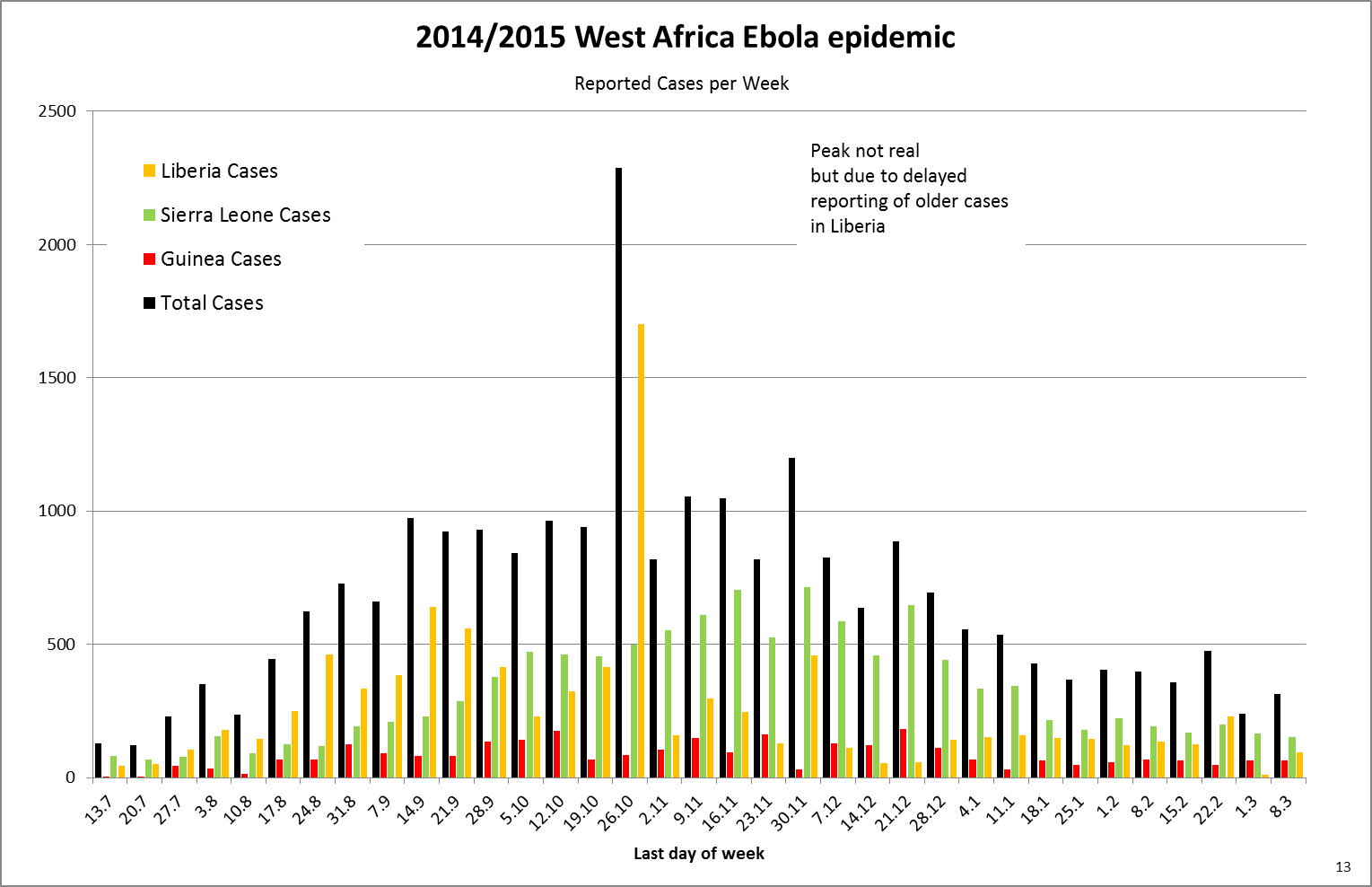
Dates in graph above listed as day/month, from Wiki.
http://en.wikipedia.org/wiki/Ebola_virus_epidemic_in_West_Africa
If contact tracing requires isolating 10-20 people with whom 1,000 new cases per week had had contact, this would mean isolating and monitoring some 10,000 to 20,000 people, just for these new infections. Nonetheless, due to the decrease in the number of new cases in Liberia, there has been some reported success with stopping new emerging clusters of Ebola in isolated areas by isolation of exposed contacts.
Estimates of Future Impact of Ebola Epidemic
It appears that the number of new Ebola cases per week has "stabilized" at approximately 1,000 cases per week.
Patient Zero
It is believed that the epidemic began when a two year old child was infected with Ebola through unknown means and died on December 6th, 2013, in a small village in Guinea which is also geographically close to the borders of both Sierra Leone and Liberia.
Transmission of this Ebola strain
Though it is believed that this Ebola strain only spread through direct contact with contaminated bodily fluids of symptomatic patients or corpses of Ebola victims, past experiments on the virus have indicated that Ebola may be passed through large droplets from some animals to others, without direct physical contact. This strain of Ebola is not considered to be able to be spread by airborne transmission to human beings, though it is a highly infectious pathogen with the fluids from corpses of Ebola victims being especially infectious.
http://www.bbc.com/news/science-environment-20341423
In past weeks, some noted virologists have voiced concerns that the Ebola virus, which has been shown to be steadily mutating during transmission among people, has a very small, but finite risk, of mutating into a form of Ebola which could infect people via airborne transmission.
Sexually Transmitted Ebola Question
It has been said that it is possible that Ebola virus may remain viable in the testes up to 3 months after a person has recovered from the virus. Ebola DNA has been found in semen 7 weeks after recovering, and in vaginal fluid weeks after recovery. Some doctors believe that Ebola can remain in semen and vaginal fluid for months after infection, and these facts have prompted experts to advise against unprotected sex 3 months after recovering from Ebola.
Given that high number of Ebola survivors, perhaps as many as 6,000 Ebola survivors may be living in west africa, (with the majority infected in the last 2 months), sexual transmission of Ebola, even a small number of cases, would be an important mode of transmission to address as soon as possible.
Some believe that the sexual transmission of Ebola might already be an important mode of transmission, and such transmission might play a role in the recrudescent epidemic in Guinea.
Roadblocks to isolating and treating Ebola patients in this outbreak
Reasons for the suspected large number of unreported cases includes, but is not limited to, stigma associated with Ebola and reluctance to seek medical care, a lack of suitable hospitals beds/quarantine wards for Ebola patients in some locales, the similarity of Ebola symptoms with common endemic tropical diseases such as malaria and Lassa fever, leading to a delayed diagnosis of Ebola, the perception that doctors can do nothing to treat Ebola, and the circulating conspiracy theory that Ebola is a cover story for more nefarious activity, such as a scam by the government in Liberia to obtain international funding, or for foreign aid organizations which some believe invented the Ebola epidemic to coverup cannibalism or organ theft.
Weeks ago, in the West Point neighborhood of Liberia, hundreds of Ebola protestors raided an Ebola quarantine unit, causing approximately 30 positive Ebola patients to flee, and the protestors also looted blood and feces contaminated sheets and mattresses which may be contaminated with Ebola.
Healthcare issues in Ebola hit countries
The medical care of other serious diseases prevalent in West Africa, such as malaria, is being neglected, partly due to a lack of healthcare workers, and also due to the focus on Ebola. There were two separate Ebola outbreaks in 2012, unrelated to the present outbreak, and it is possible that at some point various aid organizations may have to deal with concurrent Ebola outbreaks in 2014 or 2015.
Deaths per day of tropical diseases prevalent in Ebola hit countries
Ebola Deaths: Unknown, officially about 100 deaths per day in the 3 countries combined, possibly 4 times higher with 400 Ebola deaths per day as many bodies are being buried without an official Ebola test.
Lassa Fever Deaths: 14
Tuberculosis: 110
Diarrhoea: 404
Malaria: 552
HIV/AIDS: 685
Obviously, these are just averages, and since malaria season has begun, and given the lack of medical care for non-Ebola conditions in some countries, the numbers for non-Ebola deaths may be significantly higher.
http://www.businessinsider.com/the-spread-of-ebola-in-west-africa-2014-8
Officially Reported Statistics through January 25th, 2015
(Actual Number of Cases and Deaths is higher, possibly two times higher, than reported numbers).
Total Number of Officially Confirmed Cases: 22,057
Total Number of Officially Confirmed Deaths: 8,795
Total Number of Officially Confirmed Cases one month ago was 19,810
Liberia: Approximately 614 (8/11), 776 (8/18), 1049 (8/26), 1307 (8/31), 1492 (9/6), 1861 (9/10), 1924 (9/14), 2188 (9/17), 2186 (9/25), 2136 (10/1), 1681 (10/12), 2795 (10/24), 2695 (11/4), 2629 (11/11), 846 (12/14), 383 (12/24), 273 (1/25) new official cases in the past month
Sierra Leone: Approximately 424 (8/11), 465 (8/18), 493 (8/26), 642 (8/31), 644 (9/6), 779 (9/10), 863 (9/14), 905 (9/17), 1094 (9/25), 1221 (10/1), 1670 (10/12), 1996 (10/24), 2073 (11/4), 2334 (11/11), 2527 (12/14), 2337 (12/28), 1315 (1/25) new official cases in the past month
Guinea: Approximately 113 (8/11), 169 (8/18), 176 (8/26), 299 (8/31), 367 (9/6), 393 (9/10), 423 (9/14), 422 (9/17), 455 (9/25), 428 (10/1), 506 (10/12), 524 (10/24), 462 (11/4), 447 (11/11), 470 (12/14), 552 (12/28), 287 (1/25) new official cases in the past month
Total Reported Cases Liberia: 8,622 (3% of these cases reported in the past month).
Total Reported Cases Sierra Leone: 10,518 (13% of these cases reported in the past month).
Total Reported Cases Guinea: 2,917 (10% of these cases reported in the past month).
The trend over the past couple months with regards to total numbers of new official Ebola cases in West Africa seems to have leveled between 800 and 1200 cases per week, however it was recently reported that the total number of officially reported cases for the region has fallen to around just 100 per week. Nonetheless, there are probably a similar number of unreported cases (possibly a hundred or more a week) as some recognized cases do not have contacts with any other known Ebola cases.
Dates in graph above listed as day/month, from Wiki.
http://en.wikipedia.org/wiki/Ebola_virus_epidemic_in_West_Africa
If contact tracing requires isolating 10-20 people with whom 1,000 new cases per week had had contact, this would mean isolating and monitoring some 10,000 to 20,000 people, just for these new infections. Nonetheless, due to the decrease in the number of new cases in Liberia, there has been some reported success with stopping new emerging clusters of Ebola in isolated areas by isolation of exposed contacts.
Estimates of Future Impact of Ebola Epidemic
It appears that the number of new Ebola cases per week has "stabilized" at approximately 1,000 cases per week.
Patient Zero
It is believed that the epidemic began when a two year old child was infected with Ebola through unknown means and died on December 6th, 2013, in a small village in Guinea which is also geographically close to the borders of both Sierra Leone and Liberia.
Transmission of this Ebola strain
Though it is believed that this Ebola strain only spread through direct contact with contaminated bodily fluids of symptomatic patients or corpses of Ebola victims, past experiments on the virus have indicated that Ebola may be passed through large droplets from some animals to others, without direct physical contact. This strain of Ebola is not considered to be able to be spread by airborne transmission to human beings, though it is a highly infectious pathogen with the fluids from corpses of Ebola victims being especially infectious.
http://www.bbc.com/news/science-environment-20341423
In past weeks, some noted virologists have voiced concerns that the Ebola virus, which has been shown to be steadily mutating during transmission among people, has a very small, but finite risk, of mutating into a form of Ebola which could infect people via airborne transmission.
Sexually Transmitted Ebola Question
It has been said that it is possible that Ebola virus may remain viable in the testes up to 3 months after a person has recovered from the virus. Ebola DNA has been found in semen 7 weeks after recovering, and in vaginal fluid weeks after recovery. Some doctors believe that Ebola can remain in semen and vaginal fluid for months after infection, and these facts have prompted experts to advise against unprotected sex 3 months after recovering from Ebola.
Given that high number of Ebola survivors, perhaps as many as 6,000 Ebola survivors may be living in west africa, (with the majority infected in the last 2 months), sexual transmission of Ebola, even a small number of cases, would be an important mode of transmission to address as soon as possible.
Some believe that the sexual transmission of Ebola might already be an important mode of transmission, and such transmission might play a role in the recrudescent epidemic in Guinea.
Roadblocks to isolating and treating Ebola patients in this outbreak
Reasons for the suspected large number of unreported cases includes, but is not limited to, stigma associated with Ebola and reluctance to seek medical care, a lack of suitable hospitals beds/quarantine wards for Ebola patients in some locales, the similarity of Ebola symptoms with common endemic tropical diseases such as malaria and Lassa fever, leading to a delayed diagnosis of Ebola, the perception that doctors can do nothing to treat Ebola, and the circulating conspiracy theory that Ebola is a cover story for more nefarious activity, such as a scam by the government in Liberia to obtain international funding, or for foreign aid organizations which some believe invented the Ebola epidemic to coverup cannibalism or organ theft.
Weeks ago, in the West Point neighborhood of Liberia, hundreds of Ebola protestors raided an Ebola quarantine unit, causing approximately 30 positive Ebola patients to flee, and the protestors also looted blood and feces contaminated sheets and mattresses which may be contaminated with Ebola.
Healthcare issues in Ebola hit countries
The medical care of other serious diseases prevalent in West Africa, such as malaria, is being neglected, partly due to a lack of healthcare workers, and also due to the focus on Ebola. There were two separate Ebola outbreaks in 2012, unrelated to the present outbreak, and it is possible that at some point various aid organizations may have to deal with concurrent Ebola outbreaks in 2014 or 2015.
Deaths per day of tropical diseases prevalent in Ebola hit countries
Ebola Deaths: Unknown, officially about 100 deaths per day in the 3 countries combined, possibly 4 times higher with 400 Ebola deaths per day as many bodies are being buried without an official Ebola test.
Lassa Fever Deaths: 14
Tuberculosis: 110
Diarrhoea: 404
Malaria: 552
HIV/AIDS: 685
Obviously, these are just averages, and since malaria season has begun, and given the lack of medical care for non-Ebola conditions in some countries, the numbers for non-Ebola deaths may be significantly higher.
http://www.businessinsider.com/the-spread-of-ebola-in-west-africa-2014-8
Last edited:
