- Joined
- Jan 23, 2007
- Messages
- 1,654
- Reaction score
- 37
I hope none of you took out student loans to pay medical school tuition. The bottom is about to fall out...
http://www.nytimes.com/2011/09/08/us/08docs.html?_r=1&src=me&ref=general
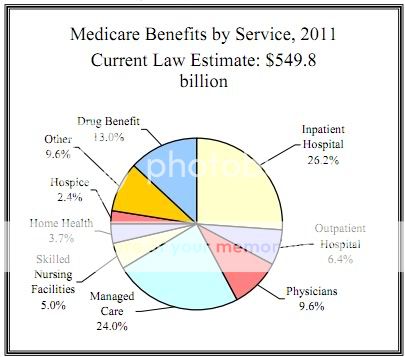
I will never understand why people think it is physician reimbursement that is contributing to increasing health care costs even though physician reimbursement goes down every year.
http://www.nytimes.com/2011/09/08/us/08docs.html?_r=1&src=me&ref=general
I will never understand why people think it is physician reimbursement that is contributing to increasing health care costs even though physician reimbursement goes down every year.