Only been an attending for a few years, but didn't EM used to pay more (either in relative or actual terms) a decade or two ago, with lower patient volumes (ie less low acuity patients)? To be honest, I would take a big pay cut to only see emergencies without the constant grind of an endless stream of patients; like the inverse of urgent careI worked 20 yrs in the community and probably did more years than most. I have worked locums in some terrible ERs. Its not like I jumped on the Unicorn Train and looking down on everyone. I bet I spent more time in the pit than you. I also understand supply and demand, so lets stop the talk of sending non urgent pts away.
But it remains that if 80% of non-ER pts didn't go to the ER, e your job would be 100x more difficult and make 1/2 of what you are now.
Imagine every pt requiring extensive work ups, admissions, critical care. Then imagine that 80% of the ERs shut down b/c there are no patients. Now imagine that you are fighting for the same job with 4 other docs. Now imagine that your pay is $120/hr because that is what someone will take.
I am also not advocating that ER is a great or even good job. I am just saying Non ER pts going to the ER makes it a better job. Prove me wrong
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
I wish patients knew what the ER was for
- Thread starter thegenius
- Start date

- Joined
- Aug 20, 2007
- Messages
- 538
- Reaction score
- 155
"it pays the bills" while, imo, being a factor in the downward quality of practicing medicine is essentially "f you, got mine." Similar to how the internet makes fun of boomers. Sure, it pays the bills but I'll take a better system in the long run if there is a way.
Gonna agree with you here. I don’t WANT to see emergent stuff all shift.I worked 20 yrs in the community and probably did more years than most. I have worked locums in some terrible ERs. Its not like I jumped on the Unicorn Train and looking down on everyone. I bet I spent more time in the pit than you. I also understand supply and demand, so lets stop the talk of sending non urgent pts away.
But it remains that if 80% of non-ER pts didn't go to the ER, e your job would be 100x more difficult and make 1/2 of what you are now.
Imagine every pt requiring extensive work ups, admissions, critical care. Then imagine that 80% of the ERs shut down b/c there are no patients. Now imagine that you are fighting for the same job with 4 other docs. Now imagine that your pay is $120/hr because that is what someone will take.
I am also not advocating that ER is a great or even good job. I am just saying Non ER pts going to the ER makes it a better job. Prove me wrong
In what other industry do people get mad at business coming through the door like ours? Especially with our looming jobs problem?
- Joined
- Oct 21, 2008
- Messages
- 6,271
- Reaction score
- 2,529
We have fast track and lobby discharge for the worried well.Study after study shows that it’s not the UC Bs that’s clogging EDs. It’s horizontal ESI 3s who need a bunch of tests and imaging and may take up an ED bed indefinitely if they’re waiting for an inpatient bed. The low acuity stuff is a doc dissatisfier in most cases but they don’t really impact flow. If you’re spending your shift seeing patients in the WR, it’s not the worried well that are the reason.
They try to get us to discharge horizontal 3s from triage before we even get a history. I won't do it.
- Joined
- Oct 21, 2008
- Messages
- 6,271
- Reaction score
- 2,529
It did not pay more two decades ago.Only been an attending for a few years, but didn't EM used to pay more (either in relative or actual terms) a decade or two ago, with lower patient volumes (ie less low acuity patients)? To be honest, I would take a big pay cut to only see emergencies without the constant grind of an endless stream of patients; like the inverse of urgent care
- Joined
- Oct 21, 2008
- Messages
- 6,271
- Reaction score
- 2,529
Patient comes, see patient. It's not that difficult.Gonna agree with you here. I don’t WANT to see emergent stuff all shift.
In what other industry do people get mad at business coming through the door like ours? Especially with our looming jobs problem?
- Joined
- Feb 4, 2017
- Messages
- 889
- Reaction score
- 1,348
Serio.It did not pay more two decades ago.
- Joined
- Nov 6, 2011
- Messages
- 3,566
- Reaction score
- 3,654
I appreciate your view because it gives you a break and it "pays the bills" (if you're paid on production).
Unfortunately, this destroys our emergency health care systems. EDs in the US, Canada, the UK, etc are drowning in surging volumes from general dumba**ery and lack of responsibility from patients to divert non-acute issues to primary care, telemedicine, urgent care, or even Googling basic first aid. God help you if your patient population skews towards entitlement/general Karen-ism.
While easy cases "pay the bills" they limit resources, increase patient mortality from boarding in the ED/overcrowding, hamper our ability to focus on truly acute/emergent issues, leads to physician and nurse burnout from high volumes -> career exodus -> understaffing -> new grads -> increased mortality and slow throughput, and taxes our healthcare system as a whole.
"But it's easy/muh RVUs $$$$" is toxically short-sighted.
I understand that your viewpoint on this is different because you have ownership stake in FSEDs. You can screen out low-acuity complaints or people that can't/won't pay/Medicaid for non-emergent BS.
Many of us do not have the luxury of working at a place that politely sends patients away after a wallet biopsy - I've worked in privately-owned FSEDs, I know how that works.
I get that you don't have to use any brain cells to prescribe a topical steroid for a rash or discharge a viral URI, but EDs in most English-speaking first world countries are drowning in this **** and patients and our family members ARE the ones that suffer when there are no beds, they don't see a doctor in a timely manner for an emergent problem, or there aren't enough nurses to work because most EDs are such a dumpster fire these days.
What's sad is that in my experience the doctors with this mindset are often the first to expect special treatment and immediate high quality care for their loved ones with private rooms, quick tests, and specialty consultations while letting everyone else wait 5-10 hrs to be seen in a hall bed.
- Joined
- Nov 6, 2011
- Messages
- 3,566
- Reaction score
- 3,654
Only been an attending for a few years, but didn't EM used to pay more (either in relative or actual terms) a decade or two ago, with lower patient volumes (ie less low acuity patients)? To be honest, I would take a big pay cut to only see emergencies without the constant grind of an endless stream of patients; like the inverse of urgent care
So the pay was basically the same but remember with inflation 300/hr was like 400/hr in today's money.
I know many older attendings that were able to afford 3-4 million dollar houses within a few years after residency.
- Joined
- Jul 6, 2008
- Messages
- 3,477
- Reaction score
- 5,977
You have two choice of ERs. Both pay $250/hr, same benefits, same pay package, 2pph, same everything
Hospital #1 - You see all Level 5 pts, 60% admission, 25% CC, procedure heavy.
Hospital #2 - You see 10% level 5, 90% UC stuff.
Job 1 will burn you out in 6 months. Job 2 will allow you to work for 20 yrs.
Hospital #1 - You see all Level 5 pts, 60% admission, 25% CC, procedure heavy.
Hospital #2 - You see 10% level 5, 90% UC stuff.
Job 1 will burn you out in 6 months. Job 2 will allow you to work for 20 yrs.
- Joined
- Jul 27, 2011
- Messages
- 2,257
- Reaction score
- 2,923
You have two choice of ERs. Both pay $250/hr, same benefits, same pay package, 2pph, same everything
Hospital #1 - You see all Level 5 pts, 60% admission, 25% CC, procedure heavy.
Hospital #2 - You see 10% level 5, 90% UC stuff.
Job 1 will burn you out in 6 months. Job 2 will allow you to work for 20 yrs.
i would pick job 2 all day every day.
I would not want every single patient to be critical. I need my easy wins - in fact, it’s a major bummer when i go into a sore throat room only to find that it’s going to be a work up because of an abscess. Id much rather have that patient who you swab and send home.
But maybe I’m just lazy and like being paid for the least amount of work 🤣
The ideal shift would be 1 pph of sore throats and low acuity stuff where i still get paid exactly the same $$$/hour as a 2-3 pph shift with high volume and high acuity.
It is the chill, relaxing, low acuity and low volume days that actually recharge me.
- Joined
- Dec 19, 2020
- Messages
- 741
- Reaction score
- 1,593
I only wish I could have the acuity for the example in hospital #1. High acuity and critical care are what drove me to emergency medicine. The reality of today’s EM isn’t that though. The level of acuity in example #1 doesn’t exist for most community sites, even for ones with high acuity.You have two choice of ERs. Both pay $250/hr, same benefits, same pay package, 2pph, same everything
Hospital #1 - You see all Level 5 pts, 60% admission, 25% CC, procedure heavy.
Hospital #2 - You see 10% level 5, 90% UC stuff.
Job 1 will burn you out in 6 months. Job 2 will allow you to work for 20 yrs.
Sure, if the reimbursement is the same for both then that changes the choice, but you really shouldn’t be reimbursed a flat rate instead paid for your work.
I’ve done analysis of physicians in our group who work at the higher versus lower acuity of our sites including shift types of higher and lower acuity. Those that proportionally see higher acuity make substantially more than others with proportionally lower acuity patient mixes even if they see fewer patients overall.
Give me high acuity and higher reimbursement all day long. I’ve done this for a little while even if not as long as you. The high acuity doesn’t burn me out. The onslaught of worried well with high customer service/patient satisfaction needs is what I find draining.
- Joined
- Oct 31, 2008
- Messages
- 1,784
- Reaction score
- 3,655
I only wish I could have the acuity for the example in hospital #1. High acuity and critical care are what drove me to emergency medicine. The reality of today’s EM isn’t that though. The level of acuity in example #1 doesn’t exist for most community sites, even for ones with high acuity.
Sure, if the reimbursement is the same for both then that changes the choice, but you really shouldn’t be reimbursed a flat rate instead paid for your work.
I’ve done analysis of physicians in our group who work at the higher versus lower acuity of our sites including shift types of higher and lower acuity. Those that proportionally see higher acuity make substantially more than others with proportionally lower acuity patient mixes even if they see fewer patients overall.
Give me high acuity and higher reimbursement all day long. I’ve done this for a little while even if not as long as you. The high acuity doesn’t burn me out. The onslaught of worried well with high customer service/patient satisfaction needs is what I find draining.
I couldn't agree more.
My favorite times in the ED are when I'm bouncing from a ETT to a central line to a STEMI to a chest tube to a hip reduction.
I'll take that all day.
- Joined
- May 3, 2004
- Messages
- 3,156
- Reaction score
- 3,751
Man, I'm so over the high acuity, CC and procedures. I'm 100% about Hospital #2 at my stage and currently have been fortunate to find a community gig that's in a somewhat similar environment. I've fully embraced that I'm realistically well into the latter half of my career. I'd realistically only like to be working FT for the next 10 years or so. My stress levels and BP are down. It's glorious. We have some high volume days where I might see 2.5pph but other days I might see 1.5pph. Even on the busy days, it's really easy stuff that requires zero mental power. Many 6a shifts I might not see a pt for 2-3 hours and I just do market research. I'm sure many would call it boring but I love it.
- Joined
- Jul 27, 2011
- Messages
- 2,257
- Reaction score
- 2,923
I only wish I could have the acuity for the example in hospital #1. High acuity and critical care are what drove me to emergency medicine. The reality of today’s EM isn’t that though. The level of acuity in example #1 doesn’t exist for most community sites, even for ones with high acuity.
Sure, if the reimbursement is the same for both then that changes the choice, but you really shouldn’t be reimbursed a flat rate instead paid for your work.
I’ve done analysis of physicians in our group who work at the higher versus lower acuity of our sites including shift types of higher and lower acuity. Those that proportionally see higher acuity make substantially more than others with proportionally lower acuity patient mixes even if they see fewer patients overall.
Give me high acuity and higher reimbursement all day long. I’ve done this for a little while even if not as long as you. The high acuity doesn’t burn me out. The onslaught of worried well with high customer service/patient satisfaction needs is what I find draining.
Yeah I’m straight hourly. No rvu incentive. If i see 0 patients, i get paid the same vs seeing 30.
Maybe i would have felt differently if i made more with a higher acuity and busier shift.
But nope…my best shift ever was when i saw 1 patient in 12 hours, slept 7 hours. It was a great night shift.
- Joined
- Jul 6, 2008
- Messages
- 3,477
- Reaction score
- 5,977
Give me hospital #2 where I go home refreshed, bunch of coffee breaks, and low stressed to hang out with the kids even if I was making 200 vs 300/hr.
I have worked at super high acuity places where all the 1 inch putts never make it to the main ER. They get seen by the APC up front or ferried out to the outpt clinic. Base pay for this place was $325/hr and $500/hr with bonuses. Even with the +100/hr pay, they still could not get the place staffed thus all the bonuses.
Those who say they want hospital #1 haven't experienced a stretch of shifts where people are unstable all over the place.
I have worked at super high acuity places where all the 1 inch putts never make it to the main ER. They get seen by the APC up front or ferried out to the outpt clinic. Base pay for this place was $325/hr and $500/hr with bonuses. Even with the +100/hr pay, they still could not get the place staffed thus all the bonuses.
Those who say they want hospital #1 haven't experienced a stretch of shifts where people are unstable all over the place.
- Joined
- Dec 19, 2020
- Messages
- 741
- Reaction score
- 1,593
Incorrect.Those who say they want hospital #1 haven't experienced a stretch of shifts where people are unstable all over the place.
Once you’ve run several codes at the same time, dealt with mass shootings, multi casualty drownings, or even worked at a critical access hospital needing to manage a super sick patient for a long time with no resources in bad weather because no flight out, etc., some types of EPs say, “Give me more!” Others want a pay cut and a coffee break.
Maybe not meant for true EM, resuscitation and critical care if you don’t enjoy consistent high acuity and sick patients at once. Perhaps better suited for acute primary care or urgent care.
- Joined
- Jul 6, 2008
- Messages
- 3,477
- Reaction score
- 5,977
Padawan has lots to learn. Learn you will soon. Soon you will be coming back to thread with tail between legs.
- Joined
- Nov 21, 2003
- Messages
- 3,355
- Reaction score
- 2,833
So the "give me more" group is going to break down into:Incorrect.
Once you’ve run several codes at the same time, dealt with mass shootings, multi casualty drownings, or even worked at a critical access hospital needing to manage a super sick patient for a long time with no resources in bad weather because no flight out, etc., some types of EPs say, “Give me more!” Others want a pay cut and a coffee break.
Maybe not meant for true EM, resuscitation and critical care if you don’t enjoy consistent high acuity and sick patients at once. Perhaps better suited for acute primary care or urgent care.
1)docs working in a relatively frictionless system where they're not dealing with dead kids, meth'ed out rage zombies, consultants being paid to take call who refuse to care for patients, and interminable delays for diagnostic testing on every patient.
2) adrenaline junkies who enjoy the chaos and trauma because their biology or upbringing wired them to need high conflict environments.
3) new docs looking to prove their competence to the world and/or who haven't attenuated to the level of stimulation the ED provides.
Theoretically we're in medicine to help the patient. All the things that you imply are exciting in your list above represent scenarios that are really suboptimal for the patient. Watching a 40 yr old dying in front of his wife as his aorta continues to slowly rip open while getting refusals from every CT surgeon in a city with more than 80 hospitals isn't fun or exciting. It doesn't make you a better doc or a better person. It's kinda weird (although I can understand it) to want to be in a situation were patients do worse than they should so that you get to feel like a hero on the ones you "save".
- Joined
- Jan 22, 2012
- Messages
- 858
- Reaction score
- 1,512
In what other industry are businesses forced to take on “customers” whether or not they pay and with no legal protections on top of that?In what other industry do people get mad at business coming through the door like ours? Especially with our looming jobs problem?
- Joined
- Mar 1, 2010
- Messages
- 24,350
- Reaction score
- 36,601
Study after study shows that it’s not the UC Bs that’s clogging EDs. It’s horizontal ESI 3s who need a bunch of tests and imaging and may take up an ED bed indefinitely if they’re waiting for an inpatient bed. The low acuity stuff is a doc dissatisfier in most cases but they don’t really impact flow. If you’re spending your shift seeing patients in the WR, it’s not the worried well that are the reason.
what I think the studies miss is they are measuring bed dwell time, not physician "work required".
The honest truth is, because of documentation demands, a bull**** ass complaint and a going to the ICU sepsis require similar time. If I'm being fully honest, the tooth pain requires more time and resources becuse a lot of the sepsis patients are non verbal and its just a full exam in silence. The low acuity person requires a full chitchat that takes longer than a body exam. Then they both require the same amount of paperwork time.
sick patients (as long as they dont require procedures) and not sick patients require similar actual physician work times and if im busy writing my 5th currently asymptomatic "I had the sniffles when I woke up but they're gone now" note of the day I am delayed picking up the next person. And I can discharge that person immediately and do their chart later, or DC them when my note is done....but unless I'm a masochist, i'm not leaving without the note done and i'm basing my day and productivity around getting that note done BEFORE my shift is up. Theyre sucking up physician resources, even if they could be vacating a bed quickly.
- Joined
- Jul 6, 2008
- Messages
- 3,477
- Reaction score
- 5,977
Your idealism is commendable but not fixed in reality.Incorrect.
Once you’ve run several codes at the same time, dealt with mass shootings, multi casualty drownings, or even worked at a critical access hospital needing to manage a super sick patient for a long time with no resources in bad weather because no flight out, etc., some types of EPs say, “Give me more!” Others want a pay cut and a coffee break.
Maybe not meant for true EM, resuscitation and critical care if you don’t enjoy consistent high acuity and sick patients at once. Perhaps better suited for acute primary care or urgent care.
Everything sounds exciting but you are finishing a grueling 10 hr shift, got everything buttoned up 15 min before your shift ends and ready to go home. Ambulance pulls up, crashing patient comes in. As you love this, I am sure you will be jumping on this 2 hr grenade work up. Yeah, reality will hit.
- Joined
- Mar 1, 2010
- Messages
- 24,350
- Reaction score
- 36,601
I'll weigh in on this whole job #1 vs Job #2:
I recently changed jobs and went from high acuity around the clock (obviously not the exaggerated #1 example, but a LOT more level 5s and procedure than the national average) for x $/hr. worked at the state of the art hospital and it looked beautiful and I had most resources I could a sk for. I felt fulfilled and loved it and every day left me exhausted but so damn happy that I was doing pretty much what I trained for and was paid above local going rates for it. Went home with an extra hour of charting to do most days, but on slightly less than half of days I would get lucky enough to finish them all before I go. The gripes I have are about the insane demands put on me and how its a struggle to keep up with them without making a mistake.
I switched to cruddy cash strapped hospital desperate to keep nursing levels appropriate. Because of that, the sick patients just dont tend to come here. Obviously super sick and living nearby comes here, but ambulances that think they can drive past us with their sick but not crashing patients go elsewhere. And I get it. We have a robust (ROBUST) population of chronically kind-of-ill people who are loyal and show up and lots of worried well. Plenty of peds too, which are just never really that sick except in the rare occasion where they are super sick. The volume (per provider) is essentially the same, but the acuity is mostly quite low. The pay is basically x+10 $/hr. Its a minor raise, but largely we are talking similar pay. BUT THE LIFESTYLE IS AMAZING. I'm always done with my charts. I come home happy for a different reason - because I have energy to see my family and act like a human being not an exhausted and worn out tool. The gripes I have are about running out of the reagent for x test or lacking y device that would have been useful. Its never about the job itself and I have no concerns that the demands are putting my license at risk. Its all slow pitches right down the center all day except for 2 or 3 fastballs that you clearly see coming.
I want to go back to job 1 as a part timer. Do a few shifts a month that still thrill me. But just a few, I like my life at job #2. I'm totally okay, even just 6-7 years out of residency, easing into some easy job that pays well. Its much more thankless, but my wife and my sanity thank me. We call it semi-retired work.
I recently changed jobs and went from high acuity around the clock (obviously not the exaggerated #1 example, but a LOT more level 5s and procedure than the national average) for x $/hr. worked at the state of the art hospital and it looked beautiful and I had most resources I could a sk for. I felt fulfilled and loved it and every day left me exhausted but so damn happy that I was doing pretty much what I trained for and was paid above local going rates for it. Went home with an extra hour of charting to do most days, but on slightly less than half of days I would get lucky enough to finish them all before I go. The gripes I have are about the insane demands put on me and how its a struggle to keep up with them without making a mistake.
I switched to cruddy cash strapped hospital desperate to keep nursing levels appropriate. Because of that, the sick patients just dont tend to come here. Obviously super sick and living nearby comes here, but ambulances that think they can drive past us with their sick but not crashing patients go elsewhere. And I get it. We have a robust (ROBUST) population of chronically kind-of-ill people who are loyal and show up and lots of worried well. Plenty of peds too, which are just never really that sick except in the rare occasion where they are super sick. The volume (per provider) is essentially the same, but the acuity is mostly quite low. The pay is basically x+10 $/hr. Its a minor raise, but largely we are talking similar pay. BUT THE LIFESTYLE IS AMAZING. I'm always done with my charts. I come home happy for a different reason - because I have energy to see my family and act like a human being not an exhausted and worn out tool. The gripes I have are about running out of the reagent for x test or lacking y device that would have been useful. Its never about the job itself and I have no concerns that the demands are putting my license at risk. Its all slow pitches right down the center all day except for 2 or 3 fastballs that you clearly see coming.
I want to go back to job 1 as a part timer. Do a few shifts a month that still thrill me. But just a few, I like my life at job #2. I'm totally okay, even just 6-7 years out of residency, easing into some easy job that pays well. Its much more thankless, but my wife and my sanity thank me. We call it semi-retired work.
- Joined
- Dec 19, 2010
- Messages
- 10,255
- Reaction score
- 13,584
Patients not knowing what the ED is for, is as synonymous with Emergency Medicine as eternity is long.
- Joined
- Aug 29, 2006
- Messages
- 1,640
- Reaction score
- 2,009
Hourly pay rates were similar or better 10 years ago but inflation wasn't this bad and housing costs (the big one) were much lower.Only been an attending for a few years, but didn't EM used to pay more (either in relative or actual terms) a decade or two ago, with lower patient volumes (ie less low acuity patients)? To be honest, I would take a big pay cut to only see emergencies without the constant grind of an endless stream of patients; like the inverse of urgent care
- Joined
- Feb 21, 2021
- Messages
- 348
- Reaction score
- 748
Hourly pay rates were similar or better 10 years ago but inflation wasn't this bad and housing costs (the big one) were much lower.
Once the feds starts cutting interest rates, watch for the housing market to sink. It is currently artificially inflated. Lots of boomers are sitting on 3% interest rates and want to downsize but cannot because of the high interest rate. Once rate goes down, they'll start selling their houses.
As long as EM hourly rate remains the same, we should have the opportunity to build wealth when that time comes.
- Joined
- Oct 31, 2008
- Messages
- 1,784
- Reaction score
- 3,655
Once the feds starts cutting interest rates, watch for the housing market to sink. It is currently artificially inflated. Lots of boomers are sitting on 3% interest rates and want to downsize but cannot because of the high interest rate. Once rate goes down, they'll start selling their houses.
As long as EM hourly rate remains the same, we should have the opportunity to build wealth when that time comes.
Might wanna check history books.
Concurrent single family home price deflation with interest rate cuts has happened twice in US history.
- Joined
- Dec 13, 2006
- Messages
- 1,773
- Reaction score
- 1,114
The housing market will go back to people bidding 40 K over asking price. The supply of houses hasn’t gone up significantly.
- Joined
- Oct 31, 2008
- Messages
- 1,784
- Reaction score
- 3,655
The housing market will go back to people bidding 40 K over asking price. The supply of houses hasn’t gone up significantly.
40k over asking would be low.
My friends are losing to all cash offers after offering 70k over asking.
- Joined
- Mar 6, 2005
- Messages
- 21,378
- Reaction score
- 17,914
Yup...happened to me recently. I was early in the process in a new location and regret not ramping up my offer.40k over asking would be low.
My friends are losing to all cash offers after offering 70k over asking.
- Joined
- Feb 21, 2021
- Messages
- 348
- Reaction score
- 748
Where is this ? A lot of major and mid-sized cities are seeing price falls.40k over asking would be low.
My friends are losing to all cash offers after offering 70k over asking.
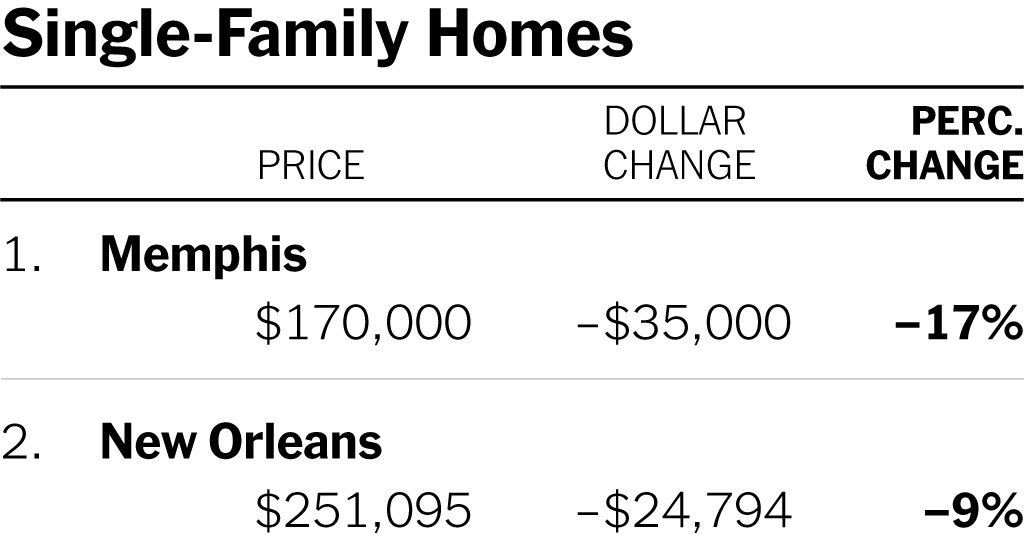
Home Prices Are Falling. Does It Matter?
Median home prices have dropped over a year, but potential buyers and sellers remain stuck in place.
- Joined
- Oct 31, 2008
- Messages
- 1,784
- Reaction score
- 3,655
Where is this ? A lot of major and mid-sized cities are seeing price falls.
Home Prices Are Falling. Does It Matter?
Median home prices have dropped over a year, but potential buyers and sellers remain stuck in place.www.nytimes.com
I think places that had huge inflationary home price drives are now coming back to earth somewhat bur the VHCOL places that characteristically are always in demand are still high.
I bought for 60 over and Zillow price has increased to the point that it is 15 over what I paid (not that Zillow means ****).
Why are people so fixated on “over” or “under” asking? It’s the marketing price. I start my eBay items at $0.01 but I don’t see people getting mad over the “crazy used PlayStation 3 market”.40k over asking would be low.
My friends are losing to all cash offers after offering 70k over asking.
I bought during the craze two years ago and had my first offer accepted. I ignored asking prices. I asked my realtor how much he thought it would go for. I offered that, and based on comps he was right on the money.
- Joined
- Dec 17, 2020
- Messages
- 422
- Reaction score
- 679
4) I’ll add a category for myself - I enjoy the challenge of fixing the place up and finding the ticking time bombs.So the "give me more" group is going to break down into:
1)docs working in a relatively frictionless system where they're not dealing with dead kids, meth'ed out rage zombies, consultants being paid to take call who refuse to care for patients, and interminable delays for diagnostic testing on every patient.
2) adrenaline junkies who enjoy the chaos and trauma because their biology or upbringing wired them to need high conflict environments.
3) new docs looking to prove their competence to the world and/or who haven't attenuated to the level of stimulation the ED
I don’t like conflict AT ALL but I am a puzzle/game fanatic and in a way it’s like a game - how well can I manage the mess to safety - CHALLENGE ACCEPTED.
I walked in last night (single coverage with a midlevel for half my shift) to 40+ in the wr, no one had been seen in 7-8 hours, the wr crowd included a complete pneumo that was starting to tension, a tumor that required sub sub specialty care, a Ludwig angina, couple NSTEMIs, a hyperkalemia missed dialysis, a patient with DTs, a septic kidney stone. I know how to persuade my consultants to help, which patients I can safely manage out front depending on the skills and personality of which nurses I have, how to maximize the beds I can wheedle out of the house sup, I cruise around with a computer and a phone between triage and waiting room and the back and the CT scanner, etc. Got everyone the care they needed, got all the rest discharged, left on time with all my charts done and 5 in the wr.
It would be easy to feel hopeless walking into that but I’d much rather do that shift than work at our freestanding and see 15 urgent care level patients. I felt exhilarated walking out of work this am because it seemed insurmountable and I got it done.
Pgy 15 .. idealism has expired lol - it’s just a better fit for me.
More power to you. If I worked at a shop where my shifts were consistently like that, I’d quit after about 2 weeks. Not because I don’t know how to triage and hustle, but just because that’s ridiculously unsafe.4) I’ll add a category for myself - I enjoy the challenge of fixing the place up and finding the ticking time bombs.
I don’t like conflict AT ALL but I am a puzzle/game fanatic and in a way it’s like a game - how well can I manage the mess to safety - CHALLENGE ACCEPTED.
I walked in last night (single coverage with a midlevel for half my shift) to 40+ in the wr, no one had been seen in 7-8 hours, the wr crowd included a complete pneumo that was starting to tension, a tumor that required sub sub specialty care, a Ludwig angina, couple NSTEMIs, a hyperkalemia missed dialysis, a patient with DTs, a septic kidney stone. I know how to persuade my consultants to help, which patients I can safely manage out front depending on the skills and personality of which nurses I have, how to maximize the beds I can wheedle out of the house sup, I cruise around with a computer and a phone between triage and waiting room and the back and the CT scanner, etc. Got everyone the care they needed, got all the rest discharged, left on time with all my charts done and 5 in the wr.
It would be easy to feel hopeless walking into that but I’d much rather do that shift than work at our freestanding and see 15 urgent care level patients. I felt exhilarated walking out of work this am because it seemed insurmountable and I got it done.
Pgy 15 .. idealism has expired lol - it’s just a better fit for me.
- Joined
- Aug 29, 2006
- Messages
- 1,640
- Reaction score
- 2,009
More power to you. If I worked at a shop where my shifts were consistently like that, I’d quit after about 2 weeks. Not because I don’t know how to triage and hustle, but just because that’s ridiculously unsafe.
Med students and residents take note - this kind of martyr complex is NOT something we should be championing. Your shop tolerates this because your group allows it.
There's "choosing lean staffing" to make more $$ (at the group's decision) and then there is UNSAFE to cut costs. This is the latter.
- Joined
- Dec 17, 2020
- Messages
- 422
- Reaction score
- 679
You and skougess are both absolutely right. It is unsafe staffing. And sadly it’s not to make $$ as we are hourly employees with no incentive to work any harder. Most of my colleagues wouldn’t have gotten to 1/3 of the sick folks and 2/3 of the ones that were ok, not because they couldn’t, but because there is no incentive to work harder, we don’t have enough staff, we aren’t set up for success and corporate does not care. No one says thank you or good job after a shift like I described. No one is criticized for doing less than what I did. We literally received an email today from our overlords explaining that our volumes don’t justify any more hours.Med students and residents take note - this kind of martyr complex is NOT something we should be championing. Your shop tolerates this because your group allows it.
There's "choosing lean staffing" to make more $$ (at the group's decision) and then there is UNSAFE to cut costs. This is the latter.
I can’t leave my current employer for {reasons}. I have the option to work at the FSED or the big house (or some other locations that are 50-200 miles away that are staffed similar to the big house) and I was just commenting on which I enjoy more. It is NOT safe and we should have more hours, but we don’t and I don’t have any control or say over that. So I make it as safe as I can and I’m being honest that I enjoy that work. Maybe Stockholm syndrome? I’m no martyr.
- Joined
- Feb 4, 2017
- Messages
- 889
- Reaction score
- 1,348
Your patients are lucky to have you. Hopefully one day you can end up in a better situation.You and skougess are both absolutely right. It is unsafe staffing. And sadly it’s not to make $$ as we are hourly employees with no incentive to work any harder. Most of my colleagues wouldn’t have gotten to 1/3 of the sick folks and 2/3 of the ones that were ok, not because they couldn’t, but because there is no incentive to work harder, we don’t have enough staff, we aren’t set up for success and corporate does not care. No one says thank you or good job after a shift like I described. No one is criticized for doing less than what I did. We literally received an email today from our overlords explaining that our volumes don’t justify any more hours.
I can’t leave my current employer for {reasons}. I have the option to work at the FSED or the big house (or some other locations that are 50-200 miles away that are staffed similar to the big house) and I was just commenting on which I enjoy more. It is NOT safe and we should have more hours, but we don’t and I don’t have any control or say over that. So I make it as safe as I can and I’m being honest that I enjoy that work. Maybe Stockholm syndrome? I’m no martyr.
Holy cow that sounds like a hard shift, and incredible if that's a "normal" day/night there. I get stressed when the solo coverage parts of my morning reach 3-4 pph during a brief window before relief shows up.
I've started moonlighting at a couple CAH in the areas. Sure it takes 30-60 minutes to drive there, and they only pay in the $160-170/hr range compared to 260ish for my main job, and I sometimes have to admit patients for skilled care, but you know what? Yesterday I saw one patient in a 12 hour shift making that rate about $1900 per patient which sure feels nice, I planned a family trip, updated my investing plan, and watched a whole season of Rick and Morty. I'm still keeping the main job for a few more years probably, as the benefits are good and I need to advance savings as I'm only a couple years out, but holy hell am I in the "give me less" category already.
I've started moonlighting at a couple CAH in the areas. Sure it takes 30-60 minutes to drive there, and they only pay in the $160-170/hr range compared to 260ish for my main job, and I sometimes have to admit patients for skilled care, but you know what? Yesterday I saw one patient in a 12 hour shift making that rate about $1900 per patient which sure feels nice, I planned a family trip, updated my investing plan, and watched a whole season of Rick and Morty. I'm still keeping the main job for a few more years probably, as the benefits are good and I need to advance savings as I'm only a couple years out, but holy hell am I in the "give me less" category already.
- Joined
- Feb 10, 2016
- Messages
- 3,312
- Reaction score
- 6,150
How much of these inappropriate ER visits are due to inadequate access to decent primary care? I bet that a lot of these patients would vanish if there was such access.
Maybe. It would diminish some of it. But part of the reason people come to the ED instead of their PCPs office even when their PCP can see them is we get stuff done without having to go through insurance preapproval, etc. I'm not saying that's a good thing, I'm just saying EM is largely a product of the American Healthcare system. We have a huge lack of primary care and subspecialist availability, and even when we do, the American public is not patient enough to wait on the insurance industry. So PCPs/specialists still send people to the ED anyways because "things will get done faster" and patients know that, and eventually they just cut out the middle man altogether and just come to the ED.
- Joined
- Mar 28, 2018
- Messages
- 57
- Reaction score
- 95
Agree with @gamerEMdoc. But just have to say, have been seeing a huge uptick in weak sauce PCP (and other specialty) ED referrals lately. Idk what the deal is. And not even just mid levels, I’m talking board-certified MD/DO’s. I can read their phone communication in EMR and they’re literally sending them in for non-emergent, as primary care as it gets, issues. ****ing insane.
- Joined
- Nov 21, 2003
- Messages
- 3,355
- Reaction score
- 2,833
The thing I keep in mind is that any contact with the healthcare system dramatically increases the chance of presenting to an emergency department within the next 48 hours.Agree with @gamerEMdoc. But just have to say, have been seeing a huge uptick in weak sauce PCP (and other specialty) ED referrals lately. Idk what the deal is. And not even just mid levels, I’m talking board-certified MD/DO’s. I can read their phone communication in EMR and they’re literally sending them in for non-emergent, as primary care as it gets, issues. ****ing insane.
- Joined
- Oct 31, 2008
- Messages
- 1,784
- Reaction score
- 3,655
Holy cow that sounds like a hard shift, and incredible if that's a "normal" day/night there. I get stressed when the solo coverage parts of my morning reach 3-4 pph during a brief window before relief shows up.
I've started moonlighting at a couple CAH in the areas. Sure it takes 30-60 minutes to drive there, and they only pay in the $160-170/hr range compared to 260ish for my main job, and I sometimes have to admit patients for skilled care, but you know what? Yesterday I saw one patient in a 12 hour shift making that rate about $1900 per patient which sure feels nice, I planned a family trip, updated my investing plan, and watched a whole season of Rick and Morty. I'm still keeping the main job for a few more years probably, as the benefits are good and I need to advance savings as I'm only a couple years out, but holy hell am I in the "give me less" category already.
Which season?
I'm so far behind.
Been meaning to catch up but I'm knee deep in Elden Ring right now.
- Joined
- Oct 4, 2002
- Messages
- 804
- Reaction score
- 601
Actually think its the overly adequate access to fast/junk food that is more of a problem (sorry, could not resistHow much of these inappropriate ER visits are due to inadequate access to decent primary care? I bet that a lot of these patients would vanish if there was such access.
 )
)- Joined
- Jan 17, 2009
- Messages
- 552
- Reaction score
- 414
All these billy badass stories of people loving their dumpster fire ERs, I don’t think my eyes could roll any harder.
I’ve basically had two jobs since residency. One is a relatively well functioning pair of community ERs where the low acuity stuff is probably paying the bills, and help is in great supply (adequate consultants, staffing, etc.). The other job, which I recently quit, was locums at a dumpster fire ER in a small-ish out of the way town. Paradoxically the docs at my main gig are more clinically competent than the ones at the dumpster fire. Take that for what it’s worth.
I’ve basically had two jobs since residency. One is a relatively well functioning pair of community ERs where the low acuity stuff is probably paying the bills, and help is in great supply (adequate consultants, staffing, etc.). The other job, which I recently quit, was locums at a dumpster fire ER in a small-ish out of the way town. Paradoxically the docs at my main gig are more clinically competent than the ones at the dumpster fire. Take that for what it’s worth.
- Joined
- Oct 21, 2008
- Messages
- 6,271
- Reaction score
- 2,529
I happily take primary care referrals.Maybe. It would diminish some of it. But part of the reason people come to the ED instead of their PCPs office even when their PCP can see them is we get stuff done without having to go through insurance preapproval, etc. I'm not saying that's a good thing, I'm just saying EM is largely a product of the American Healthcare system. We have a huge lack of primary care and subspecialist availability, and even when we do, the American public is not patient enough to wait on the insurance industry. So PCPs/specialists still send people to the ED anyways because "things will get done faster" and patients know that, and eventually they just cut out the middle man altogether and just come to the ED.
- Joined
- Jul 6, 2008
- Messages
- 3,477
- Reaction score
- 5,977
PCP - thank you for feeding me your level 5 referrals!!!!!!
When a PCP calls to admit to the hospitalist service for hyperglycemia, it’s always a thank you. Iv/labs/cookbook care/call for admit. It’s literally 10min admission. Without pushback.
I will never understand the frustration with 1 inch puts.
Yeah, it’s more appropriate for direct admission but I got bills too and want a bag full of 1 inch level 4/5 puts.
Why do I care? I bill, get paid, I create my rvu. Win win
Much better than NH dump for weakness and confusion.
When a PCP calls to admit to the hospitalist service for hyperglycemia, it’s always a thank you. Iv/labs/cookbook care/call for admit. It’s literally 10min admission. Without pushback.
I will never understand the frustration with 1 inch puts.
Yeah, it’s more appropriate for direct admission but I got bills too and want a bag full of 1 inch level 4/5 puts.
Why do I care? I bill, get paid, I create my rvu. Win win
Much better than NH dump for weakness and confusion.
- Joined
- Jul 6, 2008
- Messages
- 3,477
- Reaction score
- 5,977
These padawans will learn soon enough.All these billy badass stories of people loving their dumpster fire ERs, I don’t think my eyes could roll any harder.
I’ve basically had two jobs since residency. One is a relatively well functioning pair of community ERs where the low acuity stuff is probably paying the bills, and help is in great supply (adequate consultants, staffing, etc.). The other job, which I recently quit, was locums at a dumpster fire ER in a small-ish out of the way town. Paradoxically the docs at my main gig are more clinically competent than the ones at the dumpster fire. Take that for what it’s worth.
Wanting more and more dumpster fire work is like a beaten spouse who doesn’t know better and thinks hubby is trying to do what’s best for them The true definition of love.
😂
- Joined
- Dec 19, 2020
- Messages
- 741
- Reaction score
- 1,593
I wish some Emergency Physicians knew what the ED was for.
We all have come across various types of EPs. The resuscitationists, the academically inclined, the clinically savvy, the adrenaline junkies, the entrepreneurs, and the PCPs in the wrong building. Some were really never meant for true EM. Sure, maybe it’s a pipe dream, but EM in its imagined form is acuity, resuscitation, critical care and life/death. Those of us with that mindset will always stay 1-2 hours after a shift to deal with someone at death’s door. Even the most jaded of us see that as very high billing and income producing. We’ve also adapted pragmatically to earn the top dollar even though we were sold the wrong bill of goods.
Some though enter EM or receive training that is geared more so with the mind sight of acute care medicine, consultation dependent, desire for shift based medicine and leaving not one minute past ‘time.’ Alternatively, these EPs are burned out on the essence of EM and really have one foot out to pasture.
We are leaders of every dumpster fire of an ED. Run your shop. Get paid for your productivity. Don’t let those that are burned out, never meant for EM in the first place, and/or in positions far removed from the current EP try to tell you that their ‘experience’ trumps yours.
We all have come across various types of EPs. The resuscitationists, the academically inclined, the clinically savvy, the adrenaline junkies, the entrepreneurs, and the PCPs in the wrong building. Some were really never meant for true EM. Sure, maybe it’s a pipe dream, but EM in its imagined form is acuity, resuscitation, critical care and life/death. Those of us with that mindset will always stay 1-2 hours after a shift to deal with someone at death’s door. Even the most jaded of us see that as very high billing and income producing. We’ve also adapted pragmatically to earn the top dollar even though we were sold the wrong bill of goods.
Some though enter EM or receive training that is geared more so with the mind sight of acute care medicine, consultation dependent, desire for shift based medicine and leaving not one minute past ‘time.’ Alternatively, these EPs are burned out on the essence of EM and really have one foot out to pasture.
We are leaders of every dumpster fire of an ED. Run your shop. Get paid for your productivity. Don’t let those that are burned out, never meant for EM in the first place, and/or in positions far removed from the current EP try to tell you that their ‘experience’ trumps yours.
- Joined
- Jan 17, 2009
- Messages
- 552
- Reaction score
- 414
Ultimately we’re all on the same team so just take this as a colleague’s opinion but to me this is quite muddled.I wish some Emergency Physicians knew what the ED was for.
We all have come across various types of EPs. The resuscitationists, the academically inclined, the clinically savvy, the adrenaline junkies, the entrepreneurs, and the PCPs in the wrong building. Some were really never meant for true EM. Sure, maybe it’s a pipe dream, but EM in its imagined form is acuity, resuscitation, critical care and life/death. Those of us with that mindset will always stay 1-2 hours after a shift to deal with someone at death’s door. Even the most jaded of us see that as very high billing and income producing. We’ve also adapted pragmatically to earn the top dollar even though we were sold the wrong bill of goods.
Some though enter EM or receive training that is geared more so with the mind sight of acute care medicine, consultation dependent, desire for shift based medicine and leaving not one minute past ‘time.’ Alternatively, these EPs are burned out on the essence of EM and really have one foot out to pasture.
We are leaders of every dumpster fire of an ED. Run your shop. Get paid for your productivity. Don’t let those that are burned out, never meant for EM in the first place, and/or in positions far removed from the current EP try to tell you that their ‘experience’ trumps yours.
I don’t think the people who don’t want to work in a dumpster fire with poorly functioning staff, angry patients and families, and unnecessarily high medicolegal risk are ‘burned out on the essence of EM’. If these are the circumstances you find yourself in every shift, I honestly wonder if your care doesn’t ultimately suffer for it.
Most of my shifts when I do have those 3 - 5 critically ill patients, I’m actually able to devote myself to them, again thanks to not working in an understaffed dumpster fire.
Similar threads
- Replies
- 112
- Views
- 8K
- Replies
- 246
- Views
- 15K