- Joined
- May 3, 2004
- Messages
- 3,156
- Reaction score
- 3,751

Private equity-back EM jobs are only 25% of the employers; you often have other options.
Simply click on the video link in the original post and fast forward to the 5:30 mark. There is no need for you to be sniffing anything.This doesn't pass the sniff test.
")
Simply click on the video link in the original post and fast forward to the 5:30 mark. There is no need for you to be sniffing anything.
A quick perusal of multiple sources cite the same statistic: 50% of EM jobs are tied to a CMG.Doesn't mean they're correct either, amigo.
25% seems too low.
 journalfeed.org
journalfeed.org
A quick perusal of multiple sources cite the same statistic: 50% of EM jobs are tied to a CMG.
Corporate Control of Emergency Departments - A Growing Monster? - JournalFeed
Spoon FeedThere is undeniable corporate influence in the practice of emergency medicine, and this could cause problems for patients or for those of us who care for them. We need to thoughtfully consider this. SourceCorporate Control of Emergency Departments: Dangers from the Growing Monster. J...
Welcome to the Emergency Room. A Wall Street Honcho Will Decide Your Treatment.
Doctors and medical experts say private equity firms and profiteering corporations are putting American lives at risk and compromising the practice of medicine.www.ineteconomics.org
However, not all CMGs are backed by private equity; about half are. Hence the 25%.
Do you have any sources to support your keen sniffer, paisano?
(See what I did there…Italian)
I’ve seen a couple of threads on this website discussing the corporate practice of medicine and private equity influence. As usual, I come to provide a contrarian perspective for your consideration.
It’s not that I disagree with the prevailing sentiment that the corporate practice of medicine is bad and needs reform - this is undeniable. I have concerns with the target of everyone’s ire and perhaps your methods.
As bad as players like TeamHeath and EMP/USACS are, I submit they are not the biggest nor most immediate threat to your longevity in this career. Private equity-back EM jobs are only 25% of the employers; you often have other options. Ladies and gentlemen of the jury, I submit that the private “nonprofit” healthcare system is a more immediate threat to your profession, and we need to make sure that actions taken to weaken private equity do not feed the gorilla in the china shop. The growth of these private and semi-public systems are a cancer, a true pustule on the ass of healthcare, that is quickly absorbing all manner of physician practices. Last I checked, they now control about 40% of healthcare jobs and show no signs of slowing down. Trust me, they behave nothing like a non-profit charity, and are as tuned into profiteering as any private equity firm. They use every anti-trust trick in the book such as physician non-compete clauses, certificate of need requirements, eminent domain, etc. to undercut competition, drive down physician salaries, and grow. Their CEOs pull salaries that you would expect to see at a major bank.
My fear is that any federal regulations that weaken these private equity groups will further strengthen the grip of private non-profits. Take a look at what happened with Atrium Heath and USACS. Atrium has quickly grown from a regional heath system, Carolinas Heath, to a national super-system with hospitals across the Southeast and Midwest. While it touts itself as a non-profit, Atrium has notoriously sued patients and physicians, engaged in deceptive billing, and vigorously lobbied politicians at all levels. When Atrium replaced USACS last month, they didn’t replace them with a SDG - they are expanding their own hospital employee group. This is nothing more than effectively eliminating yet another employer in the region and stifling competition. As much as USACS sucks, losing yet another potential employer in the Charlotte region will eventually suck more. Why? Because Atrium will control a significant portion of the EM jobs not just in Charlotte, but as far away as Winston Salem, Greensboro, High Point, and beyond.
My concern with the methods used to bring about reform are far less pressing. I appreciate that the government is often the most expedient means to bring about needed change. However, the US health system, if nothing else, seems to be the poster child for unintended consequences when Uncle Sam get deeply involved.
Many of those middle management types are former nurses though.Non-profit status for health systems is a scam.
The "profits" are never returned to the physicians and nurses who helped generate them.
Instead you have a middle management bloat of "physician leaders" who command clinical salaries to sit in meetings.
I agree and I've said this on this for for more than a decade. Any time I've tried to explain to other physicians that "non-profit" hospital systems are as much "for profit" and as greedy as any other health system, they just argue with me, never gaining understanding. It's incredibly easy for them to take massive amounts of money, redirect and rename them with accounting such that profits are no longer "profits."I submit that the private “nonprofit” healthcare system is a more immediate threat to your profession
I agree and I've said this on this for for more than a decade. Any time I've tried to explain to other physicians that "non-profit" hospital systems are as much "for profit" and as greedy as any other health system, they just argue with me, never gaining understanding. It's incredibly easy for them to take massive amounts of money, redirect and rename them with accounting such that profits are no longer "profits."
What was a "profit" is now available for CEO bonuses.
What was "profit" is now available for more administrators.
What was "profit" is now "reinvestment" for a new hospital, more administrators, more CEO/CFO salaries and more money to in whatever self-serving accounting bucket they want, to wash the stain of "profit" away.
For profit and non-profit are identical from the standpoint of directing money away from physicians, staff and patient care, without restraint.
If you don't believe me that no hospital in existence is truly not-for-profit, show me one that is "for-losses"?
You can't find one. They each want to make as much money as possible and will find every way possible to make sure as much money goes to administrators and anyone who isn't a part of the staff-patient relationship, as possible.
Non-profits are way worse than private equity for doctors. At least private equity will give you several multiples of your share value for your practice. And at least they won't lie to you and falsely claim they don't care about enriching themselves, which is exactly what the "non-profit" people will do.
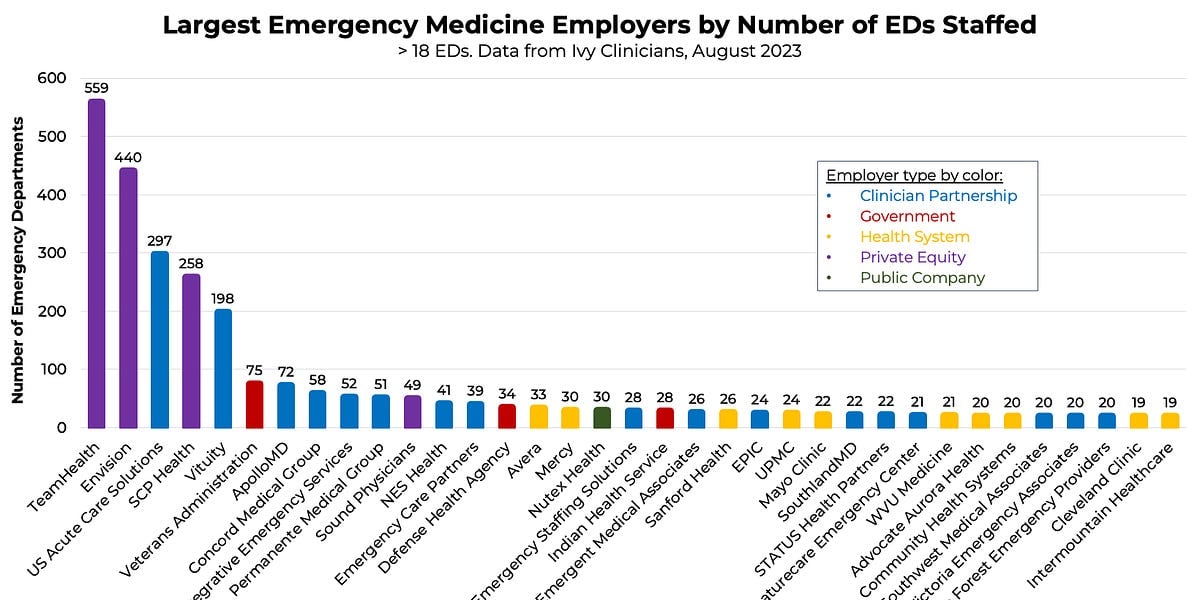
This is a good resource for the current EM employer landscape, Notice that private equity staffs 1319 of the 5705 (23.1%) EDs in the US. Heath systems staff 34% and non-equity backed partnerships about 40%. The rest are things like the VA.Shock index. You’re just wrong unfortunately. In EM (aren’t you CCM?) PE is about 70% of EM jobs or more.
 emworkforce.substack.com
emworkforce.substack.com
This is a good resource for the current EM employer landscape, Notice that private equity staffs 1319 of the 5705 (23.1%) EDs in the US. Heath systems staff 34% and non-equity backed partnerships about 40%. The rest are things like the VA.
State of the US Emergency Medicine Employer Market, Sept. 2023
Analysis based on Ivy Clinicians data.
You're seeing lots of locums @ $350/hr around you? That seems surprising, particularly at the 1.5 pph volume you posit.Last I heard, St John is a Teamhealth site with residents. Probably high volumes, high stress, mediocre pay. Probably high burnout. Probably frequent wellness meetings. Maybe it's time to just quit and do locums and actually enjoy life. So much local locums within an hour. 70k/month for 20 10-hour shifts at 1.5 pph. Sometimes it all feels like a dream until you see the checks.
Yeah, multiple sites. Can be higher or lower depending on which company you use. I've thought of quitting my full time job.You're seeing lots of locums @ $350/hr around you? That seems surprising, particularly at the 1.5 pph volume you posit.
I worked last night at the main site.
That "hate for every patient" feeling is back.
I do a great job of faking it.
I work at the freestanding tonight.
Maybe it will be better.
Probably not.
I need a vacation.
We opened our FSED the same week covid reached our state …. Lots of shifts I saw 2-5 in 12 hours .. at first I just brought cme but then I started bringing crafts and stuff .. good gig! Now that place sees 60-80/d though so no more cricut at the deskUPDATE:
EM is great when you don't see patients.
.......
At this point the non-profit megasystems are basically impossible to beat. If you go to the Wikipedia page for any small to medium sized city in the United States 90% of the time the local hospital will be the #1 employer in the area (occasionally it will be #2 or #3). Good luck getting the representatives/senators from that area to start legislating against them.
Just a couple of clarifications. First, my understanding is that the Mayo Clinic does participate in traditional Medicare (aka Original Medicare, Medicare A and B, etc.).This is where the DOJ has to step in and breakup the monopoly. Google, Apple,....next stop mega health-systems? Unlike Mayo Clinic that does not accept Medicare, these hospitals are dependent on Medicare and so can be easily brought to heel.
 www.mayoclinic.org
www.mayoclinic.org
They don’t count usacs which is PE and the 2nd largest employer. Excluding VA/IHS real numbers are 40-45% employed, 40-45% PE and 10-15% sdgs which would include Vituity. Very regional including some major cities with no sdgs.Simply click on the video link in the original post and fast forward to the 5:30 mark. There is no need for you to be sniffing anything.
Where are you seeing $350/hr?Yeah, multiple sites. Can be higher or lower depending on which company you use. I've thought of quitting my full time job.
Yeah, multiple sites. Can be higher or lower depending on which company you use. I've thought of quitting my full time job.