D
deleted171991
And even if it did, there are many factors that contribute to IVC pressure.Yes, people seem to forget that IVC diameter does not equal IVC pressure

And even if it did, there are many factors that contribute to IVC pressure.Yes, people seem to forget that IVC diameter does not equal IVC pressure
Maybe I missed it, but what was the time period between when the TTE (which proved to be inadequate) was obtained and when the TEE was performed? I'm not asking because of the whole "when the only tool you have is a hammer, everything looks like a nail" philosophy; my point is at the moment you couldn't see a high-risk valve on TTE, a TEE early would at least help focus your efforts. Thrombotic/pannus/infectious occlusion of the mitral valve prosthesis is a mechanical problem, one that you can throw all the medical management in the world at, but ultimately needs to be addressed surgically. Luckily thrombolysis took care of the problem.
And, that CVP is a poor measure of volume responsiveness.
Nice job with the case. Did you go with 100 mg TPA over 2 hours or wt. based TPA or TNKase?
Interesting case! Who pushed the tPA, your team or cards or someone else? Also, did you feel like getting the INR down before pushing?
So.. unfortunately CT surgery only available in another hospital and patient too unstable to put in the back of an ambulance.
Decided to proceed with chemical thrombolysis.
24 hours later repeat TEE shows near complete resolution of thrombus. Vaso off. Norepi down to 0.15mcg/kg/min. Continues on Milrinone. FiO2 down to 40%. Lactate on the way down.
One can't get off the Covid track with PAC.
Microthromboses in the pulmonary circulation -> increased PA pressures (same as in chronic LV failure).
Myocarditis with decreased EF -> increased PCWP.
The thing that gets off the covid track is a well-done lung ultrasound. It's unlikely to have a patient this sick without the typical subpleural lung lesions.
I've treated endocarditis patients, and I have never floated a Swan in them. Not because I don't know how to use one, but because echo (including TEE every few days) is enough for me. (Plus PAC is valuable for exactly one thing - PA pressures - and having a foreign body in a bacteremic bloodstream is not doing the patient any favors).
This patient is a classical example why PAC is almost worthless for the left heart. He had increased PCWP due to MS, not LV failure. The PCWP has gone the way of CVP and IVC diameter long time ago, in my mind, no offense.
The surgeons/fellows/residents/ED docs love checking the IVC and then asking me to check it as the intensivist. Drives me effing crazy. No, the hypotensive pt with the collapsible IVC on 100% FiO2 and so edematous their hands and feet look like balloons doesnt need more fluids! Stop looking at ONE thing and just go back to basics
My fantasy ICU would have TEEs that properly trained intensivists could throw in for dynamic assessments.
I'm only highlighting this comment to disabuse the notion that a TEE probe is something you just "throw in." A TEE is essentially a blind intubation and, honestly, the number of times you would need to do one so quickly that you couldn't wait for cardiology to come in and do it are so few and far between that I believe the time spent training CCM fellows to do them would probably be better spent on other more commonly used skills.
I disagree. Not everyone works at large academic centers where cardiologists can just pop up with a machine and a tech whenever a study is requested. At my current and previous practice, it would often be hours, if not the next day, before I can get someone up to do a TEE outside of certain high profile situations (ECMO or Impella patient). I am glad that I am trained and capable of performing my own exams, and can get a machine up from the OR quickly, should the need present itself. You are correct, though, that it is not something to take lightly. Actions based on incorrect information from an amateur echocardiographer can be devastating. This is true, however, for anything.
I'm with psychbender and FiO2 on this one.
I think TEE should be more prevalent in the ICU, and think the training is worth it. It's not per se that Cardiology won't come echo the patient's that need TEE, it's moreso that I need TEE when I need TEE. I don't want to call and wait and rationalize and ask and beg. I want the TEE. Especially in ICUs where patients are post-cardiac surgery or those that see a lot of devices/MCS, the TEE is worth its weight in gold. To not use TEE because the skills become "rusty" is a bit of a circular argument: if you don't have/like/want/feel comfortable with TEE, it doesn't get used. Then you feel rusty, so you don't use TEE. It's a fantastic tool with very little downside (at least in relation to the information obtained).
I don’t know the specifics of a PCCM fellowship but is there enough flexibility in it where you could potentially dedicate at least a couple months to echo/TEE training?
I’m not against it, just don’t think the rare instances you would need a truly emergent TEE wouldn’t be worth spending the time required To get trained and certified.
The downside is that it's a procedure that has inherent risks exacerbated by not continuing to practice the skill; it's not a circular argument. I'm sorry if you have to argue with your cardiology colleagues to get them done when you want one, but in reality, there are exceedingly few indications for an emergent TEE such that it has to be done before you can wait for a specialist to come in. And by "emergent," I don't mean "my curiosity needs satisfied and I don't feel like waiting."
I hear the claim an awful lot that someone "needs" a cath or "needs" a TEE, when in reality that's not the case. I also get the impression that people think TEE is "better" than TTE; it has its role but there are very few indications where it is the go-to study ahead of TTE.
And overall, the above misses my point. My point was that it takes a significant amount of training for even a cardiology fellow to become competent with the skill of performing a TEE, let alone interpreting the images. To me, it is a waste of time to devote that much of a CCM fellow's training to learning this skill for maybe the "count on one hand" number of times in their entire career to have to do one on their own. It's like arguing that you should learn how to do endoscopy for when you have an upper GI hemorrhage; would be nice to know how to do, but otherwise impractical in the majority of everyday practice.
Perhaps we’re saying different things, or maybe we’ll just agree to disagree.
I work in an ICU that admits medical cardiac and post-cardiac surgical patients (among others). I do LOTS of TEE. The surgeons request it. It answers many questions. The indications for TEE are actually pretty commonly met: need for echo when TTE is insufficient and inability to place patients in L lateral decubitus are chief among them.
I again disagree with you regarding waiting for cardiologists to come do an exam; I appreciate your apology, but why would I drag a cardiologist out of bed for something I’m credentialed and certified to do? I do think that me simply not wanting to wait is a good enough reason to do the exam.
I suppose we agree that we shouldn’t unnecessarily do procedures that we lack competence in. Either way, perhaps we have different training, different practices and different practice patterns. To each their own.
I think I may have misunderstood that you were credentialed to do them; what I was envisioning was the nocturnal intensivist being too impatient to wait for a study that may not necessarily be needed emergently, who may or may not have any business doing a TEE on his/her own.
There seems to be a theme among these threads that cardiologists are fighting back about doing even necessary procedures...is this that prevalent, or just a memorable minority?
I don’t know the specifics of a PCCM fellowship but is there enough flexibility in it where you could potentially dedicate at least a couple months to echo/TEE training?
I’m not against it, just don’t think the rare instances you would need a truly emergent TEE wouldn’t be worth spending the time required To get trained and certified.
 imacorinc.com
imacorinc.com
Anyone have experience with a disposable TEE probe?
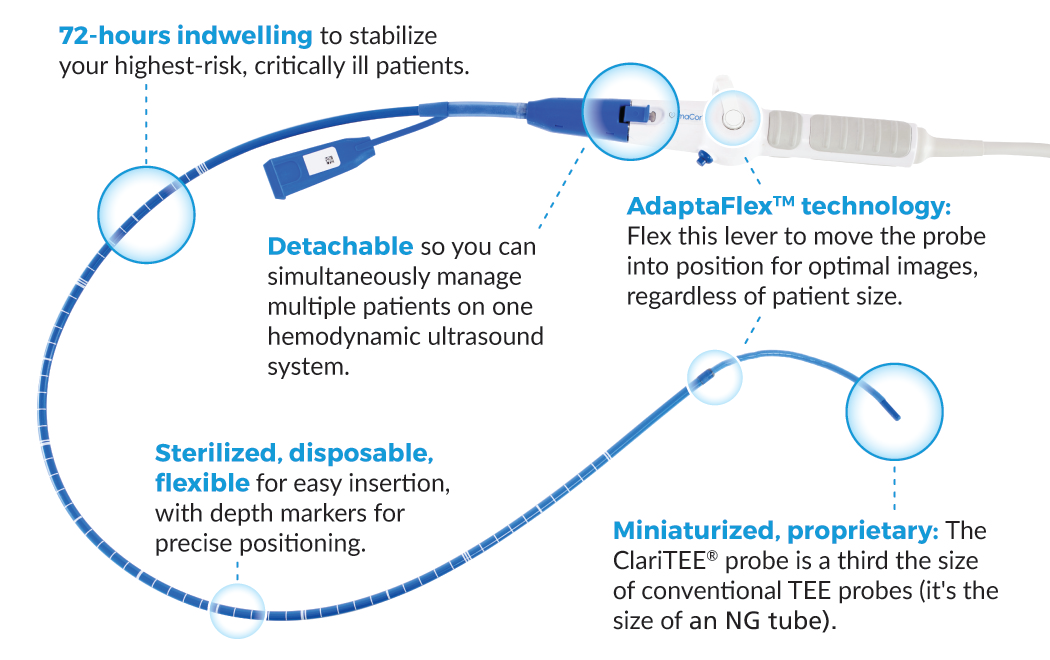
ClariTEE - Hemodynamic Ultrasound for ICU | ImaCor
Anyone leaving these in place for serial exams?
HH
Has anyone used one of those? I haven't, was just curious. From a quick look on the website seems like it's not multiplanar (fixed angle) and set up for just 3 fixed views - esophageal 4chamber, gastric short axis and IVC. Not sure it even has color flow doppler imaging? For a quick view of the LV cavity/IVC size I guess ok, but anything else (looking at various segments of the aorta, valve function, getting optimized views in setting of rotated heart/different anatomy, etc..) doesn't look like it would be that useful.
My point was that it takes a significant amount of training for even a cardiology fellow to become competent with the skill of performing a TEE, let alone interpreting the images. To me, it is a waste of time to devote that much of a CCM fellow's training to learning this skill for maybe the "count on one hand" number of times in their entire career to have to do one on their own.
An aggressive anesthesia resident could get basic certification before even starting a CCM fellowship.
+1.I'm with psychbender and FiO2 on this one.
I think TEE should be more prevalent in the ICU, and think the training is worth it. It's not per se that Cardiology won't come echo the patient's that need TEE, it's moreso that I need TEE when I need TEE. I don't want to call and wait and rationalize and ask and beg. I want the TEE. Especially in ICUs where patients are post-cardiac surgery or those that see a lot of devices/MCS, the TEE is worth its weight in gold. To not use TEE because the skills become "rusty" is a bit of a circular argument: if you don't have/like/want/feel comfortable with TEE, it doesn't get used. Then you feel rusty, so you don't use TEE. It's a fantastic tool with very little downside (at least in relation to the information obtained).

I've seen something like this at Columbia, almost 10 years ago! It was impressive.Has anyone used one of those? I haven't, was just curious. From a quick look on the website seems like it's not multiplanar (fixed angle) and set up for just 3 fixed views - esophageal 4chamber, gastric short axis and IVC. Not sure it even has color flow doppler imaging? For a quick view of the LV cavity/IVC size I guess ok, but anything else (looking at various segments of the aorta, valve function, getting optimized views in setting of rotated heart/different anatomy, etc..) doesn't look like it would be that useful.
That's because CT-CCM used to be just 18 months (no electives).Probably half of our anesthesia CCM faculty are dual cardiac trained and certified in advanced perioperative TEE. I recall being told they do about 2000 comprehensive studies per year as a group. I’d say this is the norm for high-volume, academic CVICUs.
I think that's the idea.Anyone have experience with a disposable TEE probe?
ClariTEE - Hemodynamic Ultrasound for ICU | ImaCor
Anyone leaving these in place for serial exams?
HH
Correct me if I'm wrong, but aren't anesthesia TEEs fundamentally different than cardiology TEEs. Anesthesia is trying to size valves and look at cardiac output, but they aren't assessing valvular function in quite the same way (eg MR, rheumatic vs ischemic), nor are they looking at LAA thrombus or assessing prosthetic valve function. Just because they can get the views doesn't mean they can interp what they are seeing properly when it's outside what they normally deal with.An aggressive anesthesia resident could get basic certification before even starting a CCM fellowship.
Correct me if I'm wrong, but aren't anesthesia TEEs fundamentally different than cardiology TEEs. Anesthesia is trying to size valves and look at cardiac output, but they aren't assessing valvular function in quite the same way (eg MR, rheumatic vs ischemic), nor are they looking at LAA thrombus or assessing prosthetic valve function. Just because they can get the views doesn't mean they can interp what they are seeing properly when it's outside what they normally deal with.
Correct me if I'm wrong, but aren't anesthesia TEEs fundamentally different than cardiology TEEs. Anesthesia is trying to size valves and look at cardiac output, but they aren't assessing valvular function in quite the same way (eg MR, rheumatic vs ischemic), nor are they looking at LAA thrombus or assessing prosthetic valve function. Just because they can get the views doesn't mean they can interp what they are seeing properly when it's outside what they normally deal with.
Correct me if I'm wrong, but aren't anesthesia TEEs fundamentally different than cardiology TEEs. Anesthesia is trying to size valves and look at cardiac output, but they aren't assessing valvular function in quite the same way (eg MR, rheumatic vs ischemic), nor are they looking at LAA thrombus or assessing prosthetic valve function. Just because they can get the views doesn't mean they can interp what they are seeing properly when it's outside what they normally deal with.
+1.
An intensivist should know both TTE and TEE, at least at POCUS levels. More and more, we have patients whose body habitus doesn't provide good/easy TTE windows. Especially when time is of essence, I would rather have a TEE available.
Yes, there is that intubation risk, but it's not rocket science. Ideally, every patient in shock should have one of those single-use mini-TEE probes, that look like OG tubes and allow for limited views and CO measurement, in place.
P.S. I trained at a smaller "no-name" program, hence I was trained both in TTE and TEE.
The entire science of medicine can be a Swan catheter in the hands of some providers.Might this simply be the new swan-ganz? Does or will the information actually benefit patients?? I think, like with swans, we have a bias that is does or did help, until it was studied and they didn't. I'd be interested in that study. I'm currently in the camp that everyone needing to know POCUS TEE isn't some kind of necessity for every trained intensivist. The cases when its would be "necessary" are likely too far and few, as it currently seems to me.
What is the start up cost on the POCUS single use mini-TEE probes if you have any familiarity?
The cost difference between this new device and the traditional TEE is also significant ($900 USD vs $4600 USD). Our institution saved in excess of $150,000 USD with the use of this device instead of traditional TEE.
ImaCor hTEE• Device : $65,000• Probe : $900
TTE: Prof fee $185, Technical fee $2332
TEE: Prof fee $380, Technical fee $3906
Not including technician basic after hour call in charge of $225 per echo.
The entire science of medicine can be a Swan catheter in the hands of some providers.
It seems the cost was about 65,000 for the machine and 900 per probe, back in 2012.
If you know POCUS TTE, you can learn mini-TEE on your own. I would be surprised if you need any course.That's just it though, eh? Everyone thinks they are the "some providers" who make magic out of the swan, yeah? The data simply didn't support that bias. But I'm not interested too much in re-litigating that here.
Hm. Is it all proprietary do you know? I wonder if we get a probes/set up for our two existing U/S. I need to look into it. It will be hard to get admin to agree to a new $65,000 machine right now. Cost per probe does seem to bad. Looks like there are a few courses to go to. Looks like CHEST used to have one, but no longer. Too bad.
If you know POCUS TTE, you can learn mini-TEE on your own. I would be surprised if you need any course.
The main advantage of TEE over TTE are much better and much easier to obtain images. It's just that the views are switched around. I am actually much better at (real) TEE than TTE, both learned during CCM fellowship.
Might this simply be the new swan-ganz? Does or will the information actually benefit patients?? I think, like with swans, we have a bias that is does or did help, until it was studied and they didn't. I'd be interested in that study. I'm currently in the camp that everyone needing to know POCUS TEE isn't some kind of necessity for every trained intensivist. The cases when its would be "necessary" are likely too far and few, as it currently seems to me.
What is the start up cost on the POCUS single use mini-TEE probes if you have any familiarity?
I can see where milrinone may have helped, especially if combined with a pressor. However, epi would not be high on my list of inotropes for the RV, given that it is a pulmonary vasoconstrictor.Good case. A few suggestions (having hindsight of course!) is to think more about the choice of vasopressors and inotropes, and not just throw everyone on norepi until they're maxed. In this particular caseeEven if you couldn't see the LV but you could see a crappy RV and dilated IVC with a known MV replacement, I would be starting inotropes earlier in this patient - milrinone, epi, etc. Also the description sounded like they were cold shock not warm shock, going back to basics. I would also consider some nitroglycerin if they were grossly fluid overloaded while you wait for CVVHD to work. Lastly, in someone with pseudo MS (or presumed), an esmolol drip might help to get the HR down.
What would your approach be for pressors in conjunction with milrinone? Vaso? Epi has been the inotrope of choice for RV failure post OHT at my prior institution, and I believe animal studies have shown it's beta effects outweighing any alpha induced pulmonary vasoconstriction.
Definitely a controversial subject.