While true that IM is easy to get into, it is not true that any IM program is easy to get into--the distribution of competitiveness is probably the widest of any field: residents accepted to the very top programs (e.g. UCSF, MGH) were generally very competitive for any specialty at any program, and residents accepted to e.g. mid-tier IM programs were probably barely competitive for surgical subspecialties, and some residents accepted to ****ty community programs probably shouldn't be doctors.
The thing that drove me into IM is the flexibility. Even with just residency completed, clinical jobs range from primary care (business hours + lots of follow-up and off-hour work) to hospitalist work (shiftwork, one week heavy one week off, nice salary). You can easily pursue academia and teach, do basic science research, do clinical research, or do public health research. You can subspecialize into something that's very outpatient such as Endocrine or something that is inpatient and procedure-heavy like Critical Care. If you look around your medical school and hospital, you might find that a large proportion of the high-up administration were originally from medicine, and I don't think that is a coincidence. For myself personally, I have a business / entrepreneurial background, so taking a field with a short residency, still adding a ton of value to myself to e.g. a healthcare investment boutique, and being able to pursue part-time clinical work just made the most sense.
I think any field will get boring--at least, I get bored easily and have never done anything for 40 years. Medicine offers the most diversification of my career. Lastly, the world is changing at a rapid pace, and who knows what e.g. Radiology will look like in 20 years? Or Pathology? Or Dermatology? --or Internal Medicine, but with the diversity of the field you're protected a little bit.
It is absolutely true that general medicine faces some very difficult challenges. We saddle medical students with $200k in debt and 8 years of additional schooling (+ residency) and then ask them to prioritize patient care over their own ability to pay off that debt. Sure you can argue that $150k is more than enough even then, but how can I fault anyone for pursuing fields with a significantly higher $/work-hr ratio? At the same time, the reimbursements are lower and the qualifications to get that reimbursement (documentation, patient satisfaction will be upcoming, etc.) are higher. I think a lot of general practice people feel unfairly targeted: and it's true, but the thing is that general practice represents such a large slice of the pie that a 1% cut there is so much more total savings than a 1% cut to e.g. dermatology. That's why there's so much focus.
Lastly, unlike procedure-oriented fields general medicine is a field which is most dependent on a patient's personal insight and decision-making--something that primary care physicians are expected to improve, but how do they do it? Nobody really knows except to modify reimbursements as seen above (even though there is very minimal evidence that incentivizing PROVIDERS will result in better PATIENTS, in fact there are a couple studies that show this not to be true). And frankly if we figured out how to improve people's insight and decision-making we'd corner the market in all education, not just health education. Like seriously. If you can get people to discipline themselves everyday and make good long-term decisions, you could ****ing eliminate poverty.
So is it that bad? No I think it's wonderful. But at the same time, there's enough **** going on that I don't think it a personally and financially sound decision to go into primary care without diversifying your career. Even though it's arguably what society needs the most. But --- primary care is NOT equal to internal medicine.
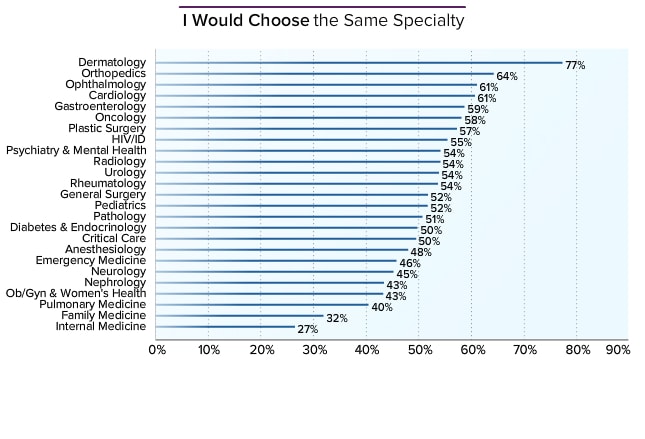
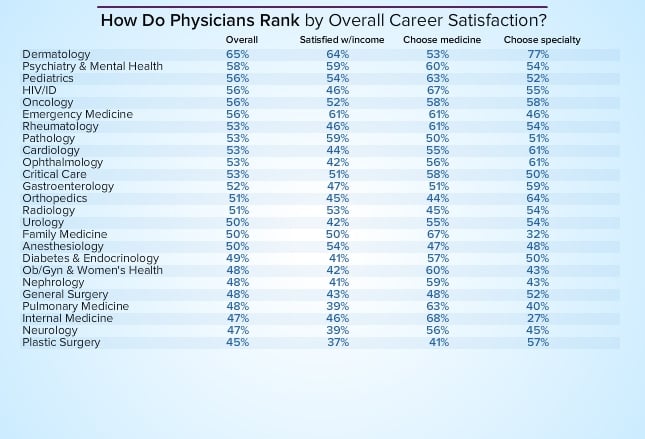
Addendum: HIV / ID is one of the higher ones up there. Clearly there are a lot of factors involved besides the $ / work-time ratio.