- Joined
- Apr 12, 2011
- Messages
- 833
- Reaction score
- 520
Anyone know of good papers comparing the two?

Anyone know of good papers comparing the two?
It's very widely used in Europe. Re PO vs IV i think we use a lot of iv because it's just easier to hang the bag when you want to rather than give it PO at an uncontrolled time on the floor.I struggle to think of any real use for IV Orfimev outside of bowel cases. At the hospital that is more liberal with us using it, I’ve gotten push back from PACU nurses about giving PO Tylenol since it’s “worse” than IV.
Like it’s Tylenol, I’m not expecting an immediate opioid-like response anyway. It’s to cut back the opioid requirements throughout the duration of action of the Tylenol.
What if case goes 10 hours? You redose in OR with IV?We did a large unpublished study with thousands in each arm. There was no difference, and we stopped using it except in rare cases. We now give most patients oral Tylenol in preop.
I don’t know if any papers to answer your actual question.
Why no pills (what's the reasoning?)We're still in the IV tylenol for everything camp (I don't make the choices). It's in several of our protocols (total joint, bariatric, colon, etc.) but really just a part of the overall ERAS / MMA effort. Our bariatric guys want no pills in pre-op. But at least for my practice, the pre-op nurses are absolutely horrible about giving PO pre-op meds right before we take the pt to the OR (typically famotidine, metoclopramide, etc.). Personally I'd prefer to give it all IV if they're not giving the PO meds on a more timely basis.
I don’t do anything for 10 hours, I’m in PP.What if case goes 10 hours? You redose in OR with IV?
TouchéI don’t do anything for 10 hours, I’m in PP.
Why no pills (what's the reasoning?)
 academic.oup.com
academic.oup.com
About a third of patient will not get to a therapeutic level with single dose 1gm of oral Tylenol because of 1rst pass metabolism.
Everyone gets a therapeutic level with single dose 1gm of IV Tylenol.
Is that worth $8? I don’t know.
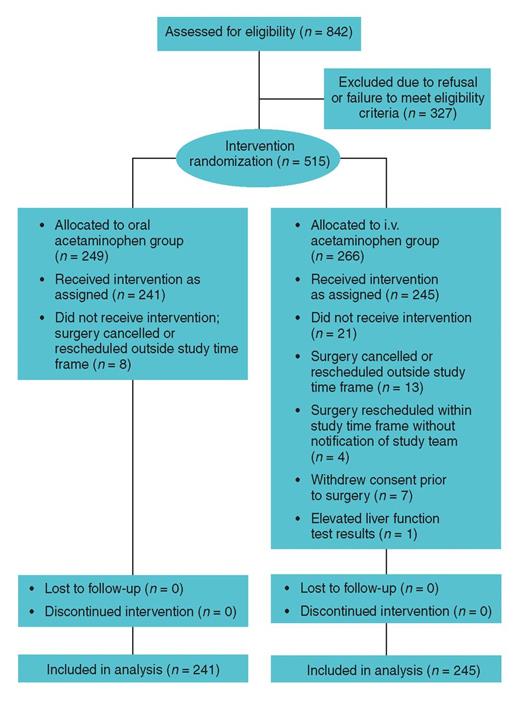
Randomized trial of oral versus intravenous acetaminophen for postoperative pain control
Purpose. Results of a study comparing pain control outcomes with preoperative oral versus intraoperative i.v. acetaminophen use in adults undergoing total
I.V. acetaminophen was not superior to oral acetaminophen in reducing postoperative nausea and vomiting, time to ambulation, time to first dose of as-needed pain medication, length of PACU stay, or total length of hospital stay.
Our hospital reports ~$30 a bottle.Real
Really? $8 per bottle. We were quoted $80-100 a bottle and our hospital did huge volumes in purchasing (40+ ORs not including fluoro procedures or GI). Hospital pharmacy quoted about the same price for suggamadex. Both overutilized and now rarely used, at least by the physicians.
About a third of patient will not get to a therapeutic level with single dose 1gm of oral Tylenol because of 1rst pass metabolism.
There are many papers on rectal acetaminophen dosing in pediatric anesthesia, you need a very large dose rectal to actually achieve a good blood level, it’s less effective than PO.Comparison to rectal tylenol?
1.2 to 1.6€/g here!$65 here - the fact that $8 and $100 are being quoted as prices for the same product is yet another huge financial problem in our healthcare system


I tend to think that absorption of PO meds before induction is complete unless you put down an OG and suck out everything. I don’t think pain should have any effect on absorption, even if there is some delayed gastric emptying.How good is GI absorption when patients get it a few minutes before going back to the OR, or immediately after surgery in PACU when patients are hurting?
Metanalysis on PO vs IV APAP are the worst. Two papers included in each of them with totally different regimens, schedules and outcomes.
there is one paper that showed that IV APAP is superior to PO in the Immediate post-op period and after controlling for various confounders.
personally I have not been convinced about the opposite and I use it almost in every case as long as the nurses did not give a preop PO dose.
Along with some lido I'm assuming
")
THAT sounds like fun ... is that after they fund your “meeting”If hear the people at Ofirmev LOVE it when you call it IV Tylenol. /s