- Joined
- Dec 13, 2005
- Messages
- 5,340
- Reaction score
- 3,621
@ragnathor I am always quite a bit deeper than that. I do test motors and sometimes do get a twitch down the leg.

I place all 6 if I'm in the first hour or two of my procedure schedule. I try to do 3 needles, but sometimes I have to do 6 bc of time.@MitchLevi that is how mine typically look. I place the right side, burn, remove and replace on the left side. Saves $30 in needle costs at the minimum.
my friend, imo, L3 mb needle placement is blocked by facet joint hypertrophy with big osteophyte extending laterally on AP view, more lateral needle placement could be helpful. wait for @bedrock and other expert's opinions, thanks.L3 MB needle looks as much as much as 2 cm too shallow, L4 MB looks maybe 0.5 cm too shallow, and L5 DPR is 3 or 4mm too shallow.
Nice L4-S1 listhesis BTW.
Also, the L3 MB needle looks a bit lateral, but if you deepen that needle it will bring the needle medially another few mm. I think you're bumping into facet rather than sneaking past it.
View attachment 372166
You likely should have started more lateral. Easiest to take needle completely out and enter more laterally. If you just try to retract, depending on how medial you were, you're going to be fighting against the facet the whole time when it can just be completely avoidedCan you be more specific in how you adjust if things look good in oblique and AP but shallow in lateral? Again usually it's the very arthritic spines I will see this - makes sense it's likely the arthritic facet. I suppose I should back up the L3 mb a couple cm and move lateral, is that the adjustment?
Bottom one sometimes I'm there sometimes I'm deeper like the others. I actually get more motor twitch there than deeper. And one else experience this?Would love some feedback. The bottom one looks a touch superficial to me but was not advanceable. Stryker probes.
I noticed you guys tend to go up and over the junction of the SAP/TP a bit. I typically have not. Curious regarding thoughts on this.
my friend, imo, L3 mb needle placement is blocked by facet joint hypertrophy with big osteophyte extending laterally on AP view, more lateral needle placement could be helpful. wait for @bedrock and other expert's opinions, thanks.
Bottom one sometimes I'm there sometimes I'm deeper like the others. I actually get more motor twitch there than deeper. And one else experience this?
Would love some feedback. The bottom one looks a touch superficial to me but was not advanceable. Stryker probes.
I noticed you guys tend to go up and over the junction of the SAP/TP a bit. I typically have not. Curious regarding thoughts on this.
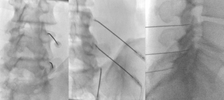
Here's a pic of one of mine I did. I had to look around to find one that wasn't severely arthritic so the needles and anatomy are easier to see.
Bilateral L4-S1. I place all needles and burn one side, remove those needles and burn the other. One image is only the right needles, but that is after I burned the left, removed those needles and I'm now burning the right.
I do 80 Celsius for 2 min, and at the 1 min mark I'll walk the needles medially or laterally 2-3mm and rotate them.
Edit - This is a patient with dementia and he's very aware of it (terrible situation). This procedure helped him walk and bend and twist. Mechanically, it helped him but there was no benefit with regard to pain. Having said that, he is unable to describe where he hurts or how bad. I hope I never get dementia.
View attachment 372167View attachment 372168View attachment 372169View attachment 372170View attachment 372171
I do.Do you place these all in the same view? I typically square off each endplate (typically no tilt or minimal tilt for L3 MB, head tilt for L4 MB and L5 DR). Not sure if it makes a true difference but it’s what I was taught.
Thanks for sharing. The only minor recommendation I could see is to drop the angle and be less perpendicular. Otherwise great depthHere's a pic of one of mine I did. I had to look around to find one that wasn't severely arthritic so the needles and anatomy are easier to see.
Bilateral L4-S1. I place all needles and burn one side, remove those needles and burn the other. One image is only the right needles, but that is after I burned the left, removed those needles and I'm now burning the right.
I do 80 Celsius for 2 min, and at the 1 min mark I'll walk the needles medially or laterally 2-3mm and rotate them.
Edit - This is a patient with dementia and he's very aware of it (terrible situation). This procedure helped him walk and bend and twist. Mechanically, it helped him but there was no benefit with regard to pain. Having said that, he is unable to describe where he hurts or how bad. I hope I never get dementia.
View attachment 372167View attachment 372168View attachment 372169View attachment 372170View attachment 372171
Please correct me if I’m wrong - Medicare will pay 50% for the other side for both joints, right?you do it based on the joints most likely to be causing your patients pain.
the reason that L3,L4 and L5 nerves are done most frequently is because the L45 and L5S1 facet joints are most likely to be pain generators.
its not because of bang for buck or financial reasons. at least not for me.
medicare allows 2 joints bilateral per session.
Agree that the bilateral L4-L5, L5-S1 are usually, not always, the worse two facet joints in the lumbar spine. This often makes sense for a 60 year old.you do it based on the joints most likely to be causing your patients pain.
the reason that L3,L4 and L5 nerves are done most frequently is because the L45 and L5S1 facet joints are most likely to be pain generators.
its not because of bang for buck or financial reasons. at least not for me.
medicare allows 2 joints bilateral per session.
For those of us buying our own needles and can't spend the money on Venom, it is my opinion there is absolutely a need to advance to anterior 1/3 of the facet. There is a clear difference in outcomes, and that depth is safe.I think op pics are fine. Key is to see multifudus twitch. No need to go to anterior. I also use venom needles. So it's going to be a big lesion.
Remember first rule of medicine do no harm.
Thank you for sharing. Is this evidence based or personal experience? just out of curiosity.I think op pics are fine. Key is to see multifudus twitch. No need to go to anterior. I also use venom needles. So it's going to be a big lesion.
Remember first rule of medicine do no harm.
Here's a pic of one of mine I did. I had to look around to find one that wasn't severely arthritic so the needles and anatomy are easier to see.
Bilateral L4-S1. I place all needles and burn one side, remove those needles and burn the other. One image is only the right needles, but that is after I burned the left, removed those needles and I'm now burning the right.
I do 80 Celsius for 2 min, and at the 1 min mark I'll walk the needles medially or laterally 2-3mm and rotate them.
Edit - This is a patient with dementia and he's very aware of it (terrible situation). This procedure helped him walk and bend and twist. Mechanically, it helped him but there was no benefit with regard to pain. Having said that, he is unable to describe where he hurts or how bad. I hope I never get dementia.
View attachment 372167View attachment 372168View attachment 372169View attachment 372170View attachment 372171
You should be perpendicular given the lesion shape.For people who use Trident do you still run parallel to the nerve or do you go perpendicular? I haven’t used those needles. I know the burn size is different. Seems like going perpendicular would really let one fly. Not sure if it would be efficacious though. Just curious.
Just looked it up, too. All I could see was Otto Octavius from Spiderman 2.Looked up the Trident! How much does that cost?? What a harpoon!
That’s why I’ve been documenting medial branch blocks and RFA to bilateral L3/4, L5/S1 for some patients. Yes it irks me to get paid less for doing more, but some patients really need it. And I suspect the overlapping innervation is exactly why they changed the reimbursement.you do it based on the joints most likely to be causing your patients pain.
medicare allows 2 joints bilateral per session.
Can you clarify what's going on in this oblique view? It looks like the tip is extending off of bone while the shaft of the needle is still contacting the SAP/TP junction. I like to get in the lateral position that you are showing. However, when I see my tip extend past the SAP/TP junction I get nervous that I'm getting too close to the root.Here's a pic of one of mine I did. I had to look around to find one that wasn't severely arthritic so the needles and anatomy are easier to see.
Bilateral L4-S1. I place all needles and burn one side, remove those needles and burn the other. One image is only the right needles, but that is after I burned the left, removed those needles and I'm now burning the right.
I do 80 Celsius for 2 min, and at the 1 min mark I'll walk the needles medially or laterally 2-3mm and rotate them.
Edit - This is a patient with dementia and he's very aware of it (terrible situation). This procedure helped him walk and bend and twist. Mechanically, it helped him but there was no benefit with regard to pain. Having said that, he is unable to describe where he hurts or how bad. I hope I never get dementia.
View attachment 372167View attachment 372168View attachment 372169View attachment 372170View attachment 372171
I have a suggestion - if you haven't done it already.what have you guys modified in private practice (compared with fellowship) to make your lumbar RFA more efficient?
I use SIS technique, 18G, 1cm curved tip cannula, lesion x 2 for 90 seconds (rotate cannula 90-100 degrees between lesions)
I have excellent RFA results but I wonder if I could change a few things to save 5 min per case, and still have similar outcomes
Thoughts on what you found improved your efficiency
What are you doing regarding needle gauge, temp/time, bevel rotation, etc?I have a suggestion - if you haven't done it already.
Take a chicken breast and take a bunch of RF needles and do some burns in it. I recently did this (I think it is worth while to repeat every once in a while to remind myself).
Notice the size of lesion vs needle size. Notice the distance past the tip. Try different temps and for different times. Try repeating the burn, or rotating the bevel and notice the difference.
I have changed how I do things based on my personal findings after these exercises.
Was the burn size different from the research paper below?I have a suggestion - if you haven't done it already.
Take a chicken breast and take a bunch of RF needles and do some burns in it. I recently did this (I think it is worth while to repeat every once in a while to remind myself).
Notice the size of lesion vs needle size. Notice the distance past the tip. Try different temps and for different times. Try repeating the burn, or rotating the bevel and notice the difference.
I have changed how I do things based on my personal findings after these exercises.
 academic.oup.com
academic.oup.com
Not really, but to see it in front of you seems more....I don't know...compelling I guess?Was the burn size different from the research paper below?
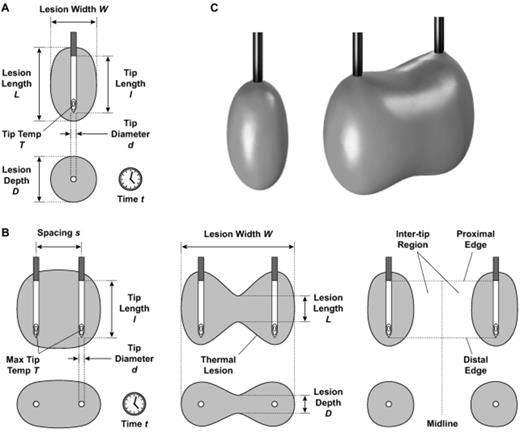
Factors That Affect Radiofrequency Heat Lesion Size
AbstractObjective. This study aims to compare radiofrequency (RF) heat lesion size across electrodes and generator settings available for interventional pa
Well, we use 18g. I wish we used 16g.What are you doing regarding needle gauge, temp/time, bevel rotation, etc?
You’re not supposed to be doing RFA at that level - unless it’s the bottom medial branch of the unfused joint? Adjusting caudal/cephalad tilt usually does the trick. Or line up the pedicle screw in gun barrel view and aim right above it and see what that gets you.On a similar note, does anyone have tips for the posterior fusions with pedicle screws…
That’s what I understand and how I do it, only if it’s the bottom or top of what I’m trying to target.You’re not supposed to be doing RFA at that level - unless it’s the bottom medial branch of the unfused joint? Adjusting caudal/cephalad tilt usually does the trick. Or line up the pedicle screw in gun barrel view and aim right above it and see what that gets you.