I think I put "uterosacral ligament" as that was the only one that extends posteriorly from the uterus.
I have a few questions of my own:
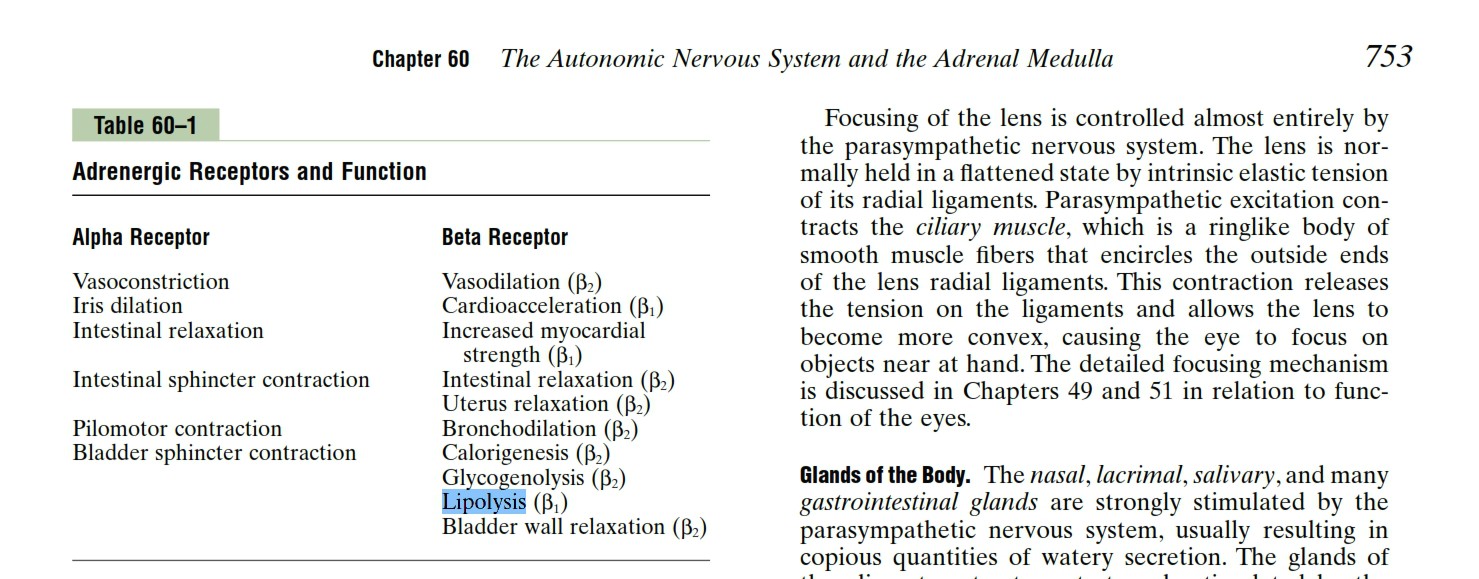
1. An investigator is studying beta2-receptors in female experimental animals. Epinephrine is injected intramuscularly into the animals, and the effects on beta2-adrenoreceptors are then observed. Which of the following physiologic effects is most likely to be observed in these animals?
A) Increased myocardial contractility
B) Internal urethral sphincter contraction
C) Lipolysis (WRONG)
D) Pilomotor contraction
E) Pupillary dilation
F) Uterine relaxation (RIGHT?)
So, I put lipolysis, which was wrong. I bet the answer is uterine relaxation, but I thought both uterine relaxation and lipolysis were possible. I dont understand why lipolysis is wrong. Is it just because you would observe uterine relaxation QUICKER than you would observe lipolysis? Or, have I finally lost it and am failing to see something obvious?
2. A 33yo woman presents with a mass in her upper outer quadrant. Examination shows 2.5 cm, hard mass. Photograph of the resected mass is shown. Which of the following characteristics best predicts this patients prognosis?
A) Degree of differentiation of the cells comprising the lesion
B) DNA content of the cells comprising the lesion
C) Lymph node involvement (RIGHT?)
D) Presence or absence of hormone receptors within the lesion (WRONG)
E) Size of the lesion
3. A 22 y/o woman comes to the physician for a follow-up examination. One year ago, she was diagnosed with a pulmonary embolism. Two years ago, she delivered a female stillborn at 23 weeks gestation. Physical examination today shows no abnormalities. Lab studies show a normal platelet count, normal prothrombin time, and increased partial thromboplastin time. The findings in this patient are most consistent with which of the following conditions?
A) Antiphospholipid antibody syndrome (RIGHT?)
B) Factor V Leiden mutation
C) Increased factor VIII (antihemophilic factor) concentration
D) Protein C deficiency (WRONG)
E) Prothrombin G20210A mutation
So, the patient has a clotting problem (DVT + miscarriage), but an increased PTT (bleeding problem) as well. I had no idea which disorder could account for both (the closest I can get is something like DIC, but that wasnt on the list). After some Google-ing, I guess its probably antiphospholipid antibody syndrome. I just want someone to confirm with an explanation, if possible. I dont think this disease is even in FA (unless Im mistaken). My Robbins pathology had only one sentence on it.
Stupid NBME 13. Did so badly.