There is ~1 NP posting in this thread, getting ganged up on by a bunch of physicians.
Part of why the NP is getting called out is because she is literally refusing to accept data that doesn't support her position and posting data that still doesn't support her position, while simultaneously attempting to paint it like it does. Intellectual dishonesty should not be tolerated no matter who it's coming from, physician, NP, nurse, PhD, or whomever.
From the looks of what’s been posted, there isn’t good evidence for any side to claim victory and honestly - would you expect there to be? And if that’s your only argument for getting a job, good luck.
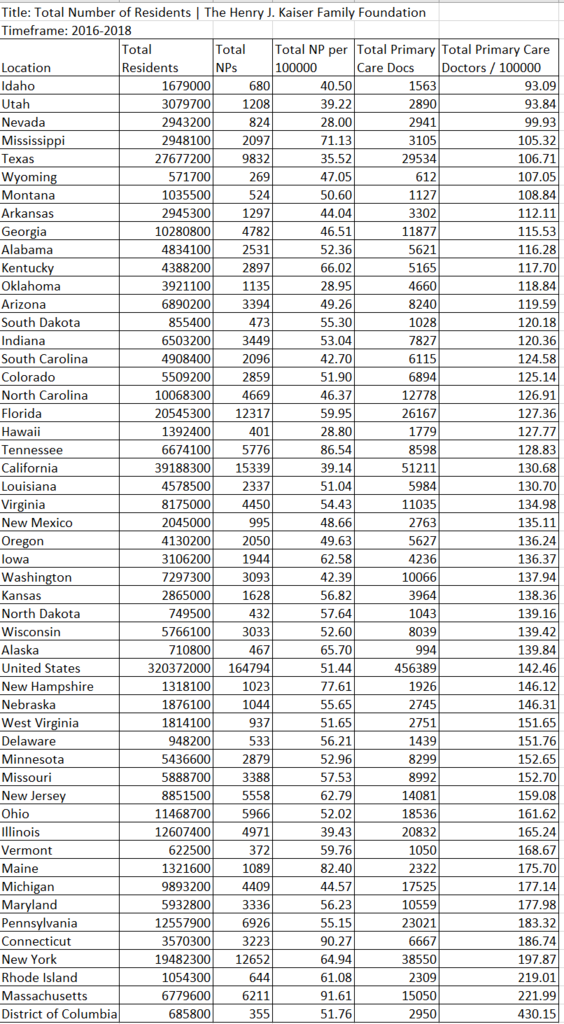
Absence of evidence isn't evidence of absence. There is no evidence NPs are equivalent to physicians outside of straightforward BP and A1C control, but there are no studies showing physicians are superior over the long term, since there are no studies that have been done over the long term. There is, however, evidence that NPs flock to urban centers and practice where there are already large numbers of physicians. If the meme that NPs are filling a gap is true, which is what the NP in this thread keeps harping on, then that flies in the face of all the data presented.
Want to protect your job from the encroachment of midlevels? Be better than them. Provide additional services that an NP wouldn’t provide. Do a fellowship. If you’re actually sure that MDs are better, you should not be insecure about this.
This is a false equivalence. The point is that NPs shouldn't be directly competing with physicians in the first place, as they have a fraction of the training and qualifications. It's like saying paralegals and attorneys should be in competition. It's absurd, but somehow it's come to be accepted as legitimate because of all the nursing propaganda.
The only real advantage that MDs have is that because we had to jump higher hurdles than they do, we’re on average smarter. But that is by no means guaranteed and intelligence isn’t everything. Most of medical school is irrelevant or redundant, so it’s not like the lack of 4 years of expensive tuition is a huge difference.
First of all, if you really think that 4 years of medical school doesn't make a difference between the quality of provider, you are delusional. Second, no one is comparing a freshly minted MD and an NP. We are talking about attendings and NPs. An attending has 4 years of medical school and 3 years of residency training, accumulating over 20,000 hours of clinical experience. NPs can graduate and start practicing with like 500 hours. There is no comparison.
A decent physician will rarely be competing with a midlevel for a spot, and a good NP with solid training and experience will easily get a job over an online degree no experience one. Put a little trust in the job market place not to make irrational decisions.
Except that game theory shows time and again that you cannot trust people to make rational decisions. Do you really think administrators will care that a new NP with an online degree is ill-equipped to handle independent practice when he costs half the price?
If you feel threatened by NPs, it’s your fault, not theirs.
I guess if I feel threatened by the enemy on deployment, it's my fault too. That mindset is absurd. Complacency kills, and complacency in healthcare politics is why we're in the situation we're in.
And maybe show a bit more civility towards
@IknowImnotadoctor - he/she’s entering enemy territory and being far more civil about it than I would be (just see my interactions with the gun nuts). Even the username is showing humility.
Calling someone out for intellectual dishonesty isn't uncivilized.
So maybe value the diversity of viewpoints instead of coming here to feel better about yourselves in a masturbatory echo chamber?
I value diversity of viewpoints when they are backed by actual data and not biased opinions.
Edit: Just to add, I actually don't think the situation is as apocalyptic as SDN makes it seem. My n is obviously small compared to the entire country, but even having worked in states where independent practice is a thing, it seems like most people still want to see the doctor when it's anything other than a URI, and sometimes even then.