- Joined
- Apr 30, 2021
- Messages
- 620
- Reaction score
- 194
Any tips on optimzing IA shoudler injections. What's your technique.
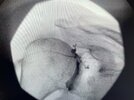
I've been having people stay supine, using x-ray to desginate shoulder joint. Then go with needle to 1/3rd way up GH joint, when hitting os, i put contrast and see spread. If not around whole joint, I move to different area.
Is there a reliable spot that guarantees good contrast spread when using fluoro?
I've been having people stay supine, using x-ray to desginate shoulder joint. Then go with needle to 1/3rd way up GH joint, when hitting os, i put contrast and see spread. If not around whole joint, I move to different area.
Is there a reliable spot that guarantees good contrast spread when using fluoro?