D
deleted950463
As title. IRs deal with a lot of ICU pts. Are there one or more things you wish to have us know about critical care?

Obstructing uretral calculus with septic shock/instability is a source control emergency, even at 3am-- please come stent it.
Cirrhotics not on warfarin with elevated INR don't usually need reversal before procedures.
Thank you for your help-- we appreciate you!
Don’t tell the ED a patient will get catheter directed lyrics for submissive PE until you have talked to the Intensivist about it first and there is an echocardiogram read from a cardiologist with a real assessment of the RV.
To be fair, a CT has approximately the same specificity and a better sensitivity for picking up RV strain than TTE. If on the CT the RV:LV ratio is decently increased, septum is flattened, there's venous contrast reflux, and the BP is only borderline normal, I'd have no problem sending to IR before the official TTE read comes back.
I cant even find methods of the study they cite.
But it doesn’t matter you need to see the RV moving or not to get an assessment of it’s FUNCTION.
There is more to the decision making process than RV strain alone. And the evidence isn't amazing for catheter based therapies in comparison to anticoagulation alone in hemodynamically stable patients. There aren't great guidelines for intermediate risk/submassive PEs and there is enormous institutional variation... I trained at one that was conservative about catheter based therapies and our patients did fine with systemic anticoagulation alone. Having some kind of multidisciplinary approach to this or a PE response team is probably best.
I don’t know if having said team is best. I know that having said team results in doing more for these patients, particularly catheter directed lytics - but there’s no data on that.
I don’t know if having said team is best. I know that having said team results in doing more for these patients, particularly catheter directed lytics - but there’s no data on that.
I feel like I’ve been able to prevent catheter lyrics if I’m involved. There are situations where I’m not involved and IR/cards/vascular have made the decision to do it in situations it seems totally unnecessary. They are financially motivated to do more.
it depends on your set up. In the setup i am familiar with the doc do not get call pay (IR docs usually do not get call pay in academia). Nor do academic IR doc get paid more on production.
if you are in an academic shop, IR is pushing for thrombolysis because we see how well it can work.
Lmgtfy
Error - Cookies Turned Off
onlinelibrary.wiley.com
And no, you don't absolutely need to see the RV "moving" with echo to say that its function has been compromised. By definition, RV dilatation to the point where it's approaching the size of the LV is always abnormal, means it's under strain, and in the case of a PE, unable to pump against the high afterload. A snapshot of flattening or bowing of the interventricular septum automatically means that RV systolic motion will be deranged from baseline. Reflux of contrast into the IVC that's extensive enough to be picked up on CT means that RVSP/PAP have become very high and the RV is under significant strain with likely distortion of the tricuspid annulus. There is enough data on many CTs (in addition to the fact that there is a big PE) to obviate the need to wait on the echo report.
I don’t know if having said team is best. I know that having said team results in doing more for these patients, particularly catheter directed lytics - but there’s no data on that.
Thank you. I did go to the link YOU originally provided. And the best way to be super snakry about googling something for someone is to use the actual LMGTFY link.
Yes. You DO need to see the RV function as a clinician. The study you cite only uses the definition of right ventricular strain (RVS) as found here in the AHA guidelines. And that is only defined as being big. The only problem with that CLINICALLY is that just being big doesn't actually often mean anything. Regardless of the size of the RV it is still working fine enough. You need to evaluate more than a simple snapshot of the size of the RV and this includes at minimum, what the patient actually looks like, are they hypoxic and or getting more hypoxic, how much obstructive hypotension is present, and is there any chemical evidence of that the RV is actually under real strain with troponin and BNP. You need to know all of this prior to committing the patient to an intervention without great evidence of great benefit (in all of these patients) in patients who simply have big RVs.
A very important part of that evaluation is the echocardiogram and how the RV is ACTUALLY functioning, not that it is just big. Most of these patient do not need their RV, even if big, more rapidly offloaded, and are fine with heparin. Starting catheter direct lytics based on CT imaging alone is practicing bad medicine.
Don't strawman me and put words into my mouth. No one was saying that we are to forgo clinical judgment or the entire clinical picture (especially in submassive where things are many times equivocal) and just make a decision based on one test. You made a statement that the TTE with an official cardiologist read is one of the things you require before telling the ED that a catheter directed lytic is appropriate. I am simply telling you and have supported with the evidence that you can make a determination of RV strain (and even significant RV compromise) as part of the clinical picture without an official TTE read back.
And I’m telling you that you absolutely actually cannot have that based on the CT scan.
RV strain is actually a fairly useless concept clinically as currently defined.
Simply saying something is big is meaningless. Ok. So what? It’s only a problem if it is a problem. And you can’t tell anything about the actual function of the RV from the CT.
You don't understand the RV, its method of muscular contraction, interventricular dependence, or its main function as a volume, not pressure, chamber if you believe that "something is big is meaningless" in regard to that structure. Being significantly enlarged is automatically pathologic, and there is a reason that "Normal Variant" is not listed as a cause of RV dilatation.. In the case of a CT where one sees significant clot burden and RV dilatation (or the other things that I mentioned earlier like IVC contrast reflux, bowed septum) we know the mechanism. You have RV pressure overload, and the RV really, really doesn't like missing out on the luxury systolic coronary perfusion that it normally receives. While "big" does matter, "how big" probably is a more important question because we see that once RV:LV ratios start getting over 1.1, people start dying a lot faster.
At the end of the day, though, we know what to do with massive PE. We also know what to do with "comfortable on RA satting 100%, SBP 138, HR 65" PEs. Submassive PEs are really the crux of the issue, and treatment algorithms take a variety of data into account, not just one data point. In the case of submassive PE, an RV:LV ratio of exactly 0.9 on a CT doesn't mean boom, go to cath lab stat. However, if a patient is uncomfortable, diaphoretic, slightly hypoxic, slightly tachycardic, small troponin leak, the RV:LV ratio is >=0.9 on CT (+- the other CT findings I mentioned), but the SBP is >90 for 15 minutes and therefore it's technically not "massive," are you going to tell me that catheter directed thrombolytics are not indicated unless you've ordered a TTE, it's been performed, and a cardiologist has read it? Is it going to change your management significantly in this patient if the TAPSE is 17mm instead of 11mm? What about if the S' is 11 instead of 9?
Now who is knocking over strawmen?! Lol.
I understand the RV fine. Just being big IS meaningless even if it "abnormal" or even "pathologic". If the patient is doing fine enough with that big RV they are doing fine enough. And YES I am going to tell you that slightly hypoxic, slightly tachycardic, small troponin leak will not go for catheter directed lytics unless there is evidence on a real time study that function is actually down. I don't care about your other strawman varibales. What does the RV actually look like.
Lol, you were the one just strawmanning my position by telling me that the CT needs to be integrated into the total picture of the patient's clinical condition (duh), but simultaneously you're trying to state that one particular test (and an often insensitive test to boot), with no explanation what precisely on that test constitutes useful information, is required to make a clinical decision. Can you describe the evidence that your patient needs to have a cardiologist interpreted TTE assessment of the RV before proceeding to cathlab, or is it merely your opinion? And if you do need that echo, what exactly defines "good" vs "bad" function vis a vis a clinical trigger to go to cathlab?
There is ZERO good data to support your approach any more than mine with a RCT.
This is EXACTLY my point. You are the one who has been saying over and over and over that you "DO" absolutely need to have a cardiologist read TTE before going to the cathlab, but there is no good evidence to support that assertion if the submassive clinical picture is bad enough. All I have pointed out is that RV dilatation on CT is essentially synonymous with some degree of RV dysfunction, and the case is even stronger when combined with septal bowing, contrast reflux into the IVC secondary to TR, or an RV:LV ratio >=1.1-1.2 instead of 0.9. I'm not incredulous that someone wouldn't take the pt to the cathlab in the scenario I described- I'm incredulous at the fact that anyone would absolutely require a cards echo to do so (or worse, that a borderline normal echo would prevent them from doing so) if the patient's HR, bnp, trop, O2 req, and CT are all consistent with a submassive requiring treatment.
Further, you are likely sidestepping this whole problematic issue of "submassive" if what you want from cards is an expert opinion of a worrisome decline in RV function. By the time a cardiologist tells you that the decline is worrisome (at least at my shop and a couple others), you've probably already reached the stage where we'd all be calling it massive and where we would have missed the window to do a lytic in a safer and timelier manner. Ultimately, what it really sounds like is that you'd rather have one more consultant for CYA purposes rather than clinical decision making.
The consultant can't cover my ass but that comment was an attempt at a weak cheap shot.
I told you why - perhaps reading comprehension isn't your best quality? - in a situation where you are talking about doing a costly procedure with the increased risks that come form a procedure that shows NO as in ZIP, ZERO group benefit for submassive patients, there needs to something more that points to enough dysfunction that the RV needs to be offloaded sooner than you will get with a heparin drip alone. I'm interested in the least harm to the patient.
I get reads on echos in 30-60 minutes. Perhaps the problem is your "shop" not my algorithm for making objective and informed decisions regarding directed lytics in the submassive PE cohort.
Ultimately, what it really sounds like is that you'd rather be a cowboy putting patients at increased risk with a procedure that shows no benefits in the entire group you are trying to treat. (This assuming the worst about each other stuff is fun).
Curious that you're trying to pull off a "no benefit" argument in a critical care forum given that we're talking about a relatively new treatment for a relatively low incidence, controversially defined condition with HUGE clinical variability, especially if the diagnosis is anywhere between "stone cold normal vitals" PE and "massive" PE. But I guess some non-CCM trained people who have no clue about the statistics of CCM studies might be fooled...if that's what you're going for. Also, you should specify "no superiority in mortality" if that's the rhetorical point you're trying make, because catheter directed therapies reduce RV strain and lower PAPs faster than A/C, have essentially equivalent mortality, and also a low procedural complication rate.
My day to day is frequently performing cardiac anesthesia, I've passed the advanced periop TEE exam, and I'm more than capable of performing and interpreting a comprehensive or POCUS TTE when I round in the unit. I don't need cardiology to give me their interpretation of an echo, but importantly, the point I'm making is that the length of time it takes the echo to come back even if you did need them is irrelevant. To get back to where we started before you began all this goalpost shifting- you initially made the claim (and in quite an absolute fact fashion) that you need to see the RV moving with echo and you need a cardiologist to read it before we can pass go. You should be very clear and state that given the dearth of evidence, this is you and your group's opinion in regard to the decision-making surrounding the treatment of potentially deteriorating submassive PE, and that other radiologic signs of RV dysfunction combined with biochemical markers and the overall clinical picture may also serve as an appropriate indication for lytics pending more data or definitive RCTs.
So many things in life age us - smoking, drinking, meth.
But only the internet can make grown adults look like children.
I shifted exactly zero goal posts in this this discussion.
If there is no objective benefit to reducing RV strain and PAP faster, then there is no reason to adventure in the risk and cost. The ends points of RV strain and PAP pressure are not meaningful simply by themselves. Show me the benefit. If you cannot, then there is no good evidence that we should be doing catheter directed lytics in all of these patients.
I think I stated that ONLY having a CT scan was not enough. You need to see the RV moving to get a sense of its real function. Just being big doesn't mean anything by the mere virtue of being big. Which was my point about the discussion regarding moving to catheter directed lytics in the first place to the question form a RADIOLOGIST about what IR could do better or different. I haven't changed or moved off the point. It is my opinion echocardiogram is necessary to make a final decision on who gets catheter directed lytics for submassive PE. It is appears it your OPINION that this evaluation of RV function is not necessary for a decision to move forward with the risk and cost associated catheter directed lytics for submassive PE. Dueling opinions. Mine simply does it's best to triage who actually needs the intervention while yours does not.
Lol you haven't shifted the goal posts? We somehow moved from the simple point of contention that echo is the be-all-end-all of RV function assessment to me having to prove that catheter directed therapy has a mortality benefit to me having to prove a negative that echo isn't worthwhile...when you are the one upon whom the burden of proof lies when you affirmatively suggest/imply that an echo will improve the eligibility criteria and probability of success of the intervention.
It's great and all that you said that ONLY having a CT scan was not enough, but as I pointed out, that was you strawmanning me because I originally said "If on the CT the RV:LV ratio is decently increased, septum is flattened, there's venous contrast reflux, and the BP is only borderline normal..." It is not a point of contention that RV function is worrisome with a dilated RV, flattened septum, and readily apparent significant tricuspid regurgitation in the setting of a CT confirmed PE. I then followed up by stating that obviously any decision is made based on the overall clinical picture, which implies that there needs to be some other supporting evidence wrt to pt's vitals, labs, oxygen requirement, appearance, etc. If you could use your reason for one second instead of just reflexively being obstinate, you'd see that I never said nor ever meant "GET CT, RV:LV 0.9, CATHLAB NOW."
If you'd like to continue strawmanning me by implying that I don't want any echo (when my actual point of contention is really the cards official read since 97% of us here are capable of a sufficient POCUS exam), or continuing to say that using radiological data as one of a multitude of data points is bad triaging, that is certainly your prerogative.
I haven’t “strawmaned” you anywhere.
You’ve made a lot of incorrect assumptions about what I’ve been saying and I do find your accusations of straw man amusingly ironic and hypocritical.
And I haven’t moved a single goal post. You were basically asking why the echo end point was so important here. If I misunderstand that question then perhaps you can clarify? My point that you seemed to be demanding an answer to was that in a situation where not all those with submissive PE benefit from catheter directed lyrics that I picked an end point of real time dynamic RV dysfunction as a reasonable point in the algorithim for patients who should have a quicker improvement in RV pressures than a heparin infusion can provide.
I'm guessing you don't know what the word means, because you have clearly misrepresented my position on CTs repeatedly just to knock down something which no one said in the first place.
And I haven't made a single incorrect assumption about what you're saying. You've made it very clear that 100% of the time you need a cardiologist-read TTE before you'd ever think of proceeding to a catheter directed lytic for submassive PE. I understand the logic and the reasoning behind it. I just disagree with the conclusion if the pt's radiological studies, clot burden, clinical picture, and labs provide enough evidence of a deteriorating submassive PE.
Ultimately, what it really sounds like is that you'd rather have one more consultant for CYA purposes rather than clinical decision making.
Haha, you guys are really going at it. It’s interesting though. But has the potential to never end.Has the unmoving object met the unstoppable force?
I admit I am not very familiar with this vector guy
Haha, you guys are really going at it. It’s interesting though. But has the potential to never end.
I lost track of who’s moving goal posts and who’s straw manning it.
I am familiar with the term straw man and I never misrepresented your position.
And yes in the case of submissive PE there needs to a real time assessment of the dynamic RV function before initiating catheter directed lyrics for the reasons now given multiple time. I suppose it matters little if it necessarily a cardiologist.
Every one of these patients has an official TTE ordered by the ED or the ICU when they're admitted.
If a patient is deteriorating that is different situation than what I've been discussing.
Haha, you guys are really going at it. It’s interesting though. But has the potential to never end.
I lost track of who’s moving goal posts and who’s straw manning it.
Weird you say that when you also said "Starting catheter direct lytics based on CT imaging alone is practicing bad medicine. " as if that were my argument.
The whole crux of this stupid argument has been which imaging modality(ies) do deteriorating submassive PE pts need before lytics. Obviously someone who has CT proven PE, a 0.08 troponin and a RV:LV of 0.9 (or a TAPSE of 14 or something) but who is stable from a hemodynamic and respiratory standpoint isn't automatically going to the cathlab....even though they technically meet the definition of a "submassive PE" (no systemic hypotension + evidence of either or both RV dysfunction or myocardial necrosis). As I said earlier, PE spans a massive (no pun intended) spectrum which ranges from normal vitals/chamber size/function/biochemical markers PE all the way to there-is-no-pulse PE.
To be very clear, it is my opinion that there are patients who are subPE but on the border who are appropriate for catheter directed lytics- without the formal read back from the TTE, assuming they have sufficient other radiologic, biochemical, and/or clinical data.
When I made the CT alone comment you were only discussing CT finding and had made no mention of other clinical factors. This was all in the context of my original statement that radiologist should not be putting in catheters for directed lytics based on CT imaging alone. Also I never said that was your argument. I said it’s bad medicine to only use that. You clearly made some assumptions there and found yourself indignant.
This discussion from my end was not about “deteriorating” patients. We were talking about who which submissive patients should get catheter directed lytics. I’m sorry you misunderstood that and again made some assumptions that clearly confused you. Trying clarifying better next time.

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
That's a good try with the "sorry you're confused" nonsense, but in the very first post I ever made about the topic I said "If on the CT the RV:LV ratio is decently increased, septum is flattened, there's venous contrast reflux, and the BP is only borderline normal, ..." From the beginning, I have intimated that the clinical picture has importance and we are talking about a borderline picture at that, even though you desperately wish (and act) as if the only statement I made was RV:LV 0.9 or BUST.
Also, I gathered from your previously stated need to have an official read back from cards that you're not really that facile or knowledgeable about echocardiography or alternative cardiac imaging modalities, but yet you bizarrely continue to disagree authoritatively with me (and without sourcing) when I tell you that RV:LV ratio, IVC contrast reflux, and abnormal septum position are synonymous with significant RV dysfunction, not to mention prognostic of adverse outcomes. Even worse, you can't even specify what it is you do want the official cardiology TTE read to say about the RV other than "worrisome." We may both be bringing our opinions to the table, but at least I can tell everyone what I'm looking for before making the clinical decision with more specificity than "worrisome."
Im sorry you were confused.
“Borderline normal” sure seems like a nice way to try and hide now. What does that mean?
I’m sure if YOU can learn echo in training I could have easily as well but I wasn’t trained with echo to more than a rough estimate on bedside echo. That is no crime. Nor is it anything to be ashamed about. You trying to beat me over the head with it Is cute but it changes nothing hero. The actual function when I decide to make my decision about treating submissive PE is important to me.
You’re presumably a critical care physician and you’re not familiar with the term “borderline” in relation to vitals, labs, tests? Yowsers, good thing I didn’t use the word “equivocal.” However, to explain it at a level simple enough for you to comprehend, traditional definitions of submassive PE use an SBP of 90 as a cutoff. A borderline normal SBP would be something like 95- technically not meeting the definition but certainly not reassuring from a clinical standpoint. Ergo, from the beginning I never advocated CT parameters as the sole criteria for taking a submassive to the cathlab.
You not being trained in echo certainly isn’t a crime. The crime is you insisting you want the cardiologist to give you an official read but the most specific he has to be about RV function to satisfy you is “worrisome.” The crime is you going around telling people who have way more experience in echo and dynamic evaluation of cardiac function that X modality is definitely better or more useful than Y, or that one “absolutely actually cannot” evaluate RV function from CT ....without providing a shred of evidence or really anything more than the opinion of you and your group.
I don't know what is so necessarily clinically unsettling about a SBP of 95.
It's no "crime" to want an up to date assessment of RV function in real time. Which is what the echo gives me.
I'm sorry you didn't like being challenged. It has clearly brought out the "best" you here complete with cries of being severely wronged. This must have been really hard for you. You can't tell me what the actual RV function is from the CT scan. There are plenty of RVs that don't look great on CT scan but look fine on echo and have otherwise fine enough clinical variables. I don't have to provide you with randomized trial or other "evidence". The RV on CT is a slice, a snap shot. It isn't an analysis of function.
If you don’t understand why a SBP of 95 isn’t the most reassuring of vitals in the context of a confirmed PE with poor CT prognostic signs, I shudder to think of how little vigilance you have for the other marginal or at-risk pts in your unit. But hey, not everyone understands the gestalt of the critically ill.
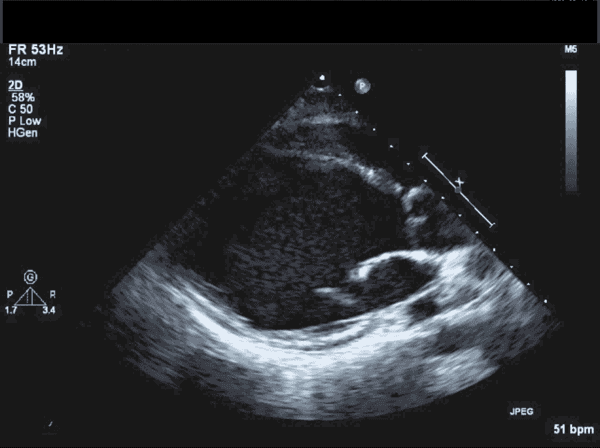
You can challenge all you want, but it’s an embarrassing attempt and utterly toothless when your reasoning begins and ends with “because I said so.” Firstly, it’s not “real time” because you have to wait for an echo tech to come and then wait for the turn around time and final read, which even under the best conditions isn’t that speedy in an evolving submassive PE who already had concerning signs on his admission CT. Secondly, it’s clear that you don’t have the foundational knowledge (aka a fking clue) to understand the implications of RV dilatation / D-shaped septum / septal bowing / interventricular dependence / presence of tricuspid regurgitation / RV pressure overload in the setting of heavy clot burden- all things which can be picked up or inferred on CT (as a side note, you also keep saying snapshot but maybe you don’t realize that rapid injection contrast studies also have some temporal information due to bolus tracking). But even if we were talking about a snapshot, look at this:
It's just a still image. There's no dynamic clips for you to get all excited about. I know you don't know much about echo, but would you like to take a guess on what this pt's LVEF is? Is there a chance on earth that it's 55%? The answer is no, and we know this based on the fundamental properties of what myocardium that is dilated to this absurd extend can do. We don't know if the LVEF is 12% or 18%, but we know it's bad. Similarly, even though our knowledge of the RV isn't as good, we know that its function is significantly compromised by gross dilation from RV pressure overload, septal distortion/bowing into the LV, and significant tricuspid regurgitation, all of which can be picked on CT and all of which are associated with a much higher risk of death in PEs. However, similarly to that dilated LV still, we don't know from a CT if the RV TAPSE is 9 or 10, but we know that a RV:LV volume ratio of 1.6:1 with septal bowing and supportive clinical signs means the function is bad enough to not need further quantitation before intervention.
I know you're so blinded but some strange desire to keep one-upping me that it probably won't matter, but just consider for a moment that your anecdote about "don't look great on CT but look fine on echo" might just be an incomplete description of what CT can tell us about ventricular function.
I find it very surprising when IR would pursue thrombolysis without input of others.
PERT team is becoming the standard of care in my opinion. Those catheter therapy can be high risk but high reward as well and there is a lack in high quality evidence because it’s an ongoing investigation. I think those procedure should involve more than IR in decision making.