Sci Rep. 2021 Dec 8;11(1):23603. doi: 10.1038/s41598-021-03081-6.
Two or four injections of platelet-rich plasma for osteoarthritic knee did not change synovial biomarkers but similarly improved clinical outcomes
Srihatach Ngarmukos 1 2, Chotetawan Tanavalee 1 3, Chavarin Amarase 1 2, Suphattra Phakham 4, Warayapa Mingsiritham 1 2, Rangsima Reantragoon 1 5, Nitigorn Leearamwat 5, Thidarat Kongkaew 5, Kittipan Tharakhet 6, Sittisak Honsawek 1 4, Sinsuda Dechsupa 4, Aree Tanavalee 7 8
Affiliations expand
PMID: 34880370 DOI: 10.1038/s41598-021-03081-6
Abstract
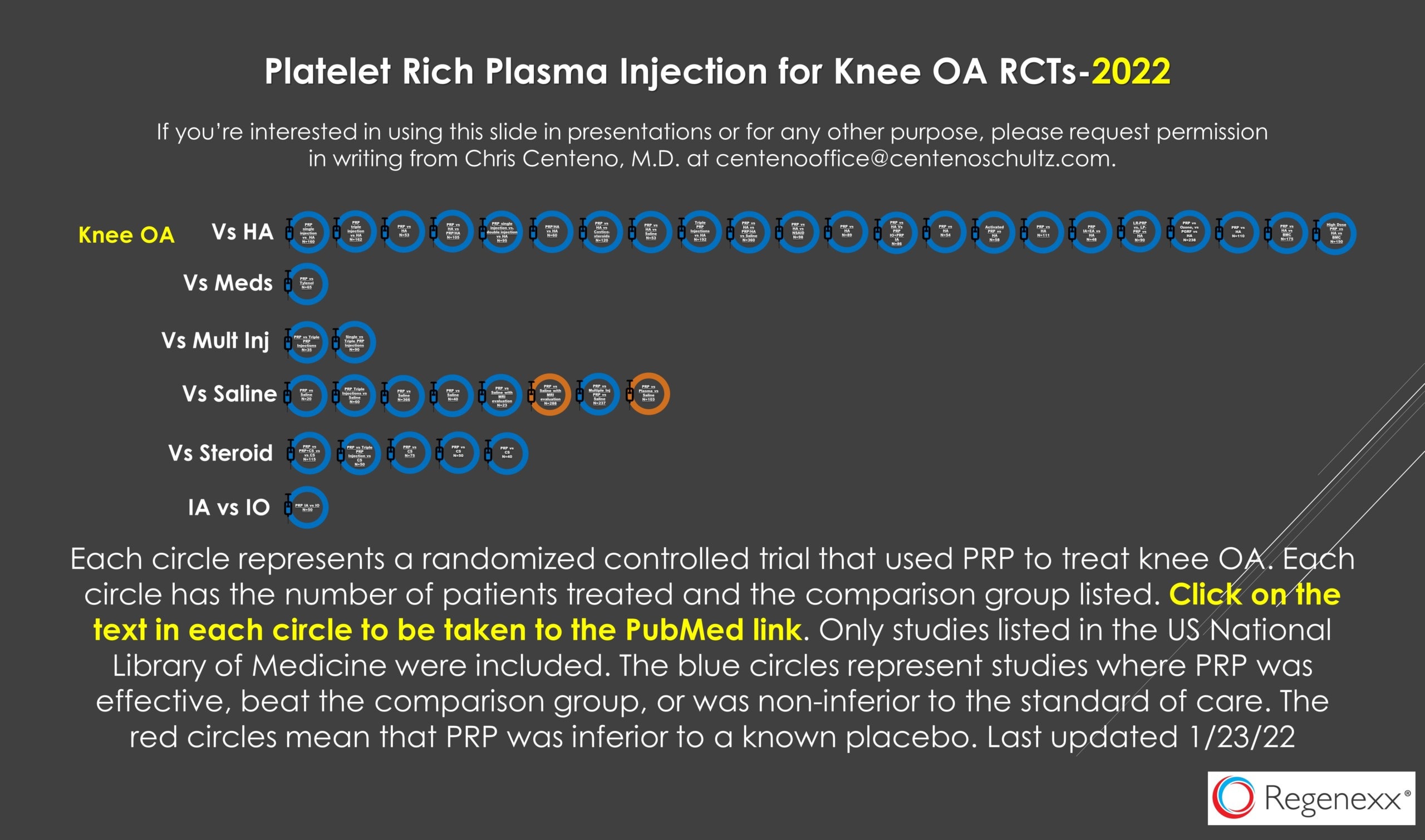
We compared two and four intra-articular injections of platelet-rich plasma (PRP) in terms of changes of synovial cytokines and clinical outcomes. One hundred twenty-five patients having knee osteoarthritis (OA) underwent PRP injections at a 6-week interval. Before each PRP injection, synovial fluid aspiration was collected for investigation. Patients were divided into two or four intra-articular PRP injections (group A and B, respectively). Changes in synovial biomarkers were compared with the baseline levels of both groups, and clinical outcomes were evaluated until one year. Ninety-four patients who had completed synovial fluid collection were included for final evaluation, 51 in group A and 43 in group B. There were no differences in mean age, gender, body mass index (BMI), and radiographic OA grading. The average platelet count and white blood cell count in PRP were 430,000/µL and 200/ µL, respectively. There were no changes of synovial inflammatory cytokines (IL-1β, IL-6, IA-17A, and TNF-alpha), anti-inflammatory cytokines (IL-4, IL-10, IL-13, and IL-1RA), and growth factors (TGF-B1, VEGF, PDGF-AA, and PDGF-BB) between baseline levels and six weeks in group A, and 18 weeks in group B. Both groups had significantly improved clinical outcomes from six weeks including visual analog scale (VAS), patient-reported outcome measures [PROMs; Western Ontario and McMaster Universities Osteoarthritis (WOMAC) Index and Short Form-12 (SF-12)], with a significant delayed improvement of performance-based measures [PBMs; time up and go (TUG), 5-time sit to stand test (5 × SST), and 3-min walk test (3-min WT)]. In conclusion, two- or four-PRP intra-articular injection at a 6-week interval for knee OA demonstrated no changes of synovial cytokines and growth factors but similarly improved clinical outcomes from 6 weeks until 1 year.
Multiple platelet-rich plasma injections are superior to single PRP injections or saline in osteoarthritis of the knee: the 2-year results of a randomized, double-blind, placebo-controlled clinical trial
Alparslan Yurtbay 1, Ferhat Say 2, Hikmet Çinka 2, Ahmet Ersoy 2
Affiliations expand
PMID: 34705072 DOI: 10.1007/s00402-021-04230-2
Abstract
Introduction: The primary purposes of this study were to prove the efficacy of PRP injection therapy on knee pain and functions by comparing patients with mild to moderate OA with a placebo control group, and also to understand the effectiveness of multiple doses compared to a single dose. It was hypothesized that PRP would lead to more favorable results than the placebo at 1, 3, 6, 12 and 24 months after treatment.
Materials and methods: 237 patients diagnosed with OA were randomly separated into 4 groups, who were administered the following: single dose of PRP (n: 62), single dose of sodium saline (NS) (n: 59), three doses of PRP (n: 63), and three doses of NS (n: 53). Clinical evaluations were made pre-treatment and at 1, 3, 6, 12 and 24 months post-treatment, using the Knee Injury and Osteoarthritis Result Score (KOOS), Kujala Patellofemoral Score, knee joint range of motion (ROM), measurements of knee circumference (KC), and mechanical axis angle (MAA) and a Visual Analog Scale (VAS) for the evaluation of pain.
Results: The better score values in the groups were recorded at 3 and 6 months. Patients treated with PRP maintained better scores at 3, 6 and 12 months compared to the NS groups (p < 0.05). Multiple doses of PRP were seen to be more effective than single-dose PRP at 6 and 12 months (p < 0.05). At the end of 24 months, there was no significant score difference across all the groups. The most positive change in scores was found in stage 2 OA, and the most positive change in ROM was in stage 3 OA patients. In the PRP groups, KC decreased more at 1 and 6 months (p < 0.05). Compared to other age groups, patients aged 51-65 years scored better at 6 months (p < 0.05). A negative correlation was determined with MAA scores (r = - 0.508, p < 0.001).
Conclusion: In comparison to the placebo (NS), leukocyte-rich PRP treatment was determined to be effective in the treatment of OA. Multiple doses of PRP increase the treatment efficacy and duration. Of all the patients treated with PRP, the best results were obtained by patients aged 51-65 years, with lower MAA, and by K/L stage 2 OA patients.