
- Joined
- Apr 22, 2007
- Messages
- 22,351
- Reaction score
- 9,010
Recently I did 2 popliteal blocks for amputation of the forefoot.
U/s guided blocks went perfectly. Yet, upon incision the patients had pain and required GA with LMA.
Solution:
Third patient presents for foot amputation.
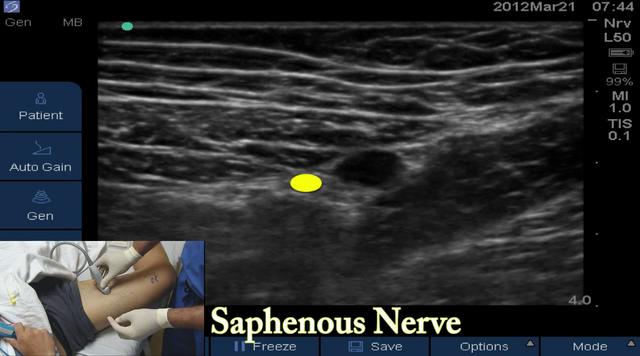
Popliteal plus adductor canal block placed
High risk patient. INR of 2.3, Plavix, etc.
EF of 15. You get the idea
Result: perfect block. Only 1 mg of midazolam for the case.
Discussion: medial side of foot and ball of big toe has saphenous nerve innervation which can be clinically significant.
U/s guided blocks went perfectly. Yet, upon incision the patients had pain and required GA with LMA.
Solution:
Third patient presents for foot amputation.
Popliteal plus adductor canal block placed
High risk patient. INR of 2.3, Plavix, etc.
EF of 15. You get the idea
Result: perfect block. Only 1 mg of midazolam for the case.
Discussion: medial side of foot and ball of big toe has saphenous nerve innervation which can be clinically significant.


")

