You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.

Because their lobbyists are better than ours
D
dyk343
I have had 3 consults this week for patients who would be best served with a BKA. All problems originating from the foot. Some of these patients I have operated on in the past (TMA, Hallux amp). One is currently septic waiting for a general surgeon to perform the consult/operation which will not be done until Monday. My attending and myself were in the hospital rounding when the ER consulted us to see if there was anything we could do... Could have been done this AM if it were not for the laws. Instead Medicare will have to pay for 1-2 more nights in the hospital.
We regularly place IM nails, Exfix, maissoneuve fractures, tibial bone graft harvest,etc etc. Why not a BKA? I feel it's a grey area.... I feel like it should be in our scope...
We regularly place IM nails, Exfix, maissoneuve fractures, tibial bone graft harvest,etc etc. Why not a BKA? I feel it's a grey area.... I feel like it should be in our scope...
More pus? No thanks.
More pus? No thanks.
I heard the Pus Bus is actually making its way to clinic as we speak. Should be there about the time you get there tomorrow. Enjoy.
D
dyk343
But what's happens when you have skin edge necrosis or another complication from your BKA? Now you have to do an AKA. Do you think a pod should be allowed to do that procedure? Where does it end?[/QUOTE said:Good point, but the same can be said with a hallux amputation. We all know those can go south quickly. Especially if they stop taking their anticoagulants
I have no idea why this reply posted this way... I cant change it..?
I have no idea why this reply posted this way... I cant change it..?
I don't think there is a gray area. You are able to put a nail (through the calc) in a tibia, take BMA and bone from the tibia, place a ring fixator, etc (and who fixes proximal fibula fxs?) as they relate and are needed to surgically correct pathology where the foot or ankle are involved.
You can't throw a tibial nail or ORIF a tibia for a shaft fx, for the same reason you can't perform a BKA. I mean sure, neither are too difficult from a technical standpoint for a pod with good training to perform. But you have to expand the scope across the board to include any and all pathology to below the knee. If you say "well we aren't asking to fix the tibia in trauma situations, just let us do BKAs" then you are right back to the whole lack of understanding of what a Podiatrist can or can't do.
Here's a funny story which Ankle Breaker already alluded to: in orientation for our new residents, a FP resident asked one of our interns who we had write prescriptions for our patients and who we sent them to for surgery...they will learn very quickly at our program that absolutely any pathology that relates to the foot or ankle is handled by our service at the hospital, and that we are the foot and ankle service within the ortho dept (and we even have a good size ortho residency program at our hospital). But the fact remains that they had literally no idea of our training or scope of practice.
Did I mention that I have no desire to do more pus than is already in our scope?
D
dyk343
I understand the tibial shaft fx and the argument there. I was thinking the same thing as the main reason we can't do them.
But if the pathology originates in the foot/ankle... shouldn't we be able to perform the procedure? We are correcting the pathology within the foot/ankle...
I can tell you the ortho and general surgeon docs in my hospital system would rather have us do the BKA's and have a hard time understanding why we can't perform the amputation when it's our patient to start with.
I know I'm pushing the limits here. But I feel it will eventually be apart of our scope. Though that will take time.
And I think I have a pretty good understanding of what legally a podiatrst can or can not do. I just don't always agree apparently. Which is why I started this thread.
(I never said we repair high fibular fxs. But I do see and treat them conservatively vs syndesmotic repair)
Edit: http://www.podiatrytoday.com/blogge...ify-gray-areas-podiatric-medicine-and-surgery
But if the pathology originates in the foot/ankle... shouldn't we be able to perform the procedure? We are correcting the pathology within the foot/ankle...
I can tell you the ortho and general surgeon docs in my hospital system would rather have us do the BKA's and have a hard time understanding why we can't perform the amputation when it's our patient to start with.
I know I'm pushing the limits here. But I feel it will eventually be apart of our scope. Though that will take time.
And I think I have a pretty good understanding of what legally a podiatrst can or can not do. I just don't always agree apparently. Which is why I started this thread.
(I never said we repair high fibular fxs. But I do see and treat them conservatively vs syndesmotic repair)
Edit: http://www.podiatrytoday.com/blogge...ify-gray-areas-podiatric-medicine-and-surgery
Last edited by a moderator:
We can technically learn to do anything. But think of it this way, if the BKA is successful then you'll be managing their stump and prosthetic complications. If the BKA fails or has wound complications, imagine what kind of practice you're gonna end up having. Are we gonna push for doing AKA next? Kindof takes us away from the specialty we've commited to begin with doesn't it? To me, the point of having ortho, plastics, or vascular do the BKA is so that they can manage their follow-up care.
D
dyk343
What happens when our TMAs go wrong? Same argument....We can technically learn to do anything. But think of it this way, if the BKA is successful then you'll be managing their stump and prosthetic complications. If the BKA fails or has wound complications, imagine what kind of practice you're gonna end up having. Are we gonna push for doing AKA next? Kindof takes us away from the specialty we've commited to begin with doesn't it? To me, the point of having ortho, plastics, or vascular do the BKA is so that they can manage their follow-up care.
Advertisement - Members don't see this ad
Don't you think it's kindof ironic for a podiatrist, a foot and ankle expert, to be managing a stump?
D
dyk343
No. Especially if the original problem originated from the foot/ankle.Don't you think it's kindof ironic for a podiatrist, a foot and ankle expert, to be managing a stump?
Don't you think it's kindof ironic for a podiatrist, a foot and ankle expert, to be managing a stump?
That reminds me of the time when I was a student rotating through one of the VAMC clinics and a patient with bilateral BKAs (well-healed) decided to go to the Podiatry clinic because the phone reminder system told him he had an appointment. We all stood there for a couple of minutes trying to decide what the heck we aimed to do until the Chief of Podiatry came in to yell at him, "Get the hell outta here!!!"
I suppose we could've checked to see that all of the nuts and bolts on his wheelchair were tight. LOL.
I suppose we could've checked to see that all of the nuts and bolts on his wheelchair were tight. LOL.
🤣
That's gold, Jerry! Gold!
No. Especially if the original problem originated from the foot/ankle.
What's next, arguing for AKA priviledges? Managing endocarditis because it came from an infected foot ulcer? Vertebral body debridement due to hematogenous spread osteomyelitis due to that same foot ulcer? Spine surgery for scoliosis that's causing ankle pain? I'll be happy to send you my patients who have asymptomatic feet but swear they are causing their knee, hip, or back pain. There's got to be a line drawn at some point...
D
dyk343
What's next, arguing for AKA priviledges? Managing endocarditis because it came from an infected foot ulcer? Vertebral body debridement due to hematogenous spread osteomyelitis due to that same foot ulcer? Spine surgery for scoliosis that's causing ankle pain? I'll be happy to send you my patients who have asymptomatic feet but swear they are causing their knee, hip, or back pain. There's got to be a line drawn at some point...
You're bringing up ludicrous situations to manage your point.
My point is we're experts below the knee and especially the foot/ankle. After my 1st year of residency I scrubbed two Pilon fractures that involved midshaft of the tibia. Despite a midshaft fracture, these cases were 100% in our scope of practice because it involved the ankle joint. With that said I feel we should be able to do BKAs if the problem originated within the foot or ankle.
I guess I am alone on this issue... Well except for the general surgeons at the hospital who keep asking why we can't do them and are not fond of our consults for BKAs. Or the ED docs who keep paging us over and over again for diabetic infections that have no chance for salvage and me having to explain to them again and again that we can not do BKAs /there is nothing I can offer the patient. Most importantly our patient's who want to stay with their current doctor who they have been undergoing limb salvage with for years (we do a ton of charcot recon here) and have developed a strong rapport with.
50 years ago podiatrists were scoffed at for requesting any surgical privileges. Not that long ago we never had a shot at touching the ankle. Today that has all changed.
Anything is possible. I think we see osseous work to the tibial tuberosity in my career timeline. In the mean time, i'm more than happy to scrub BKAs with the general surgeons at my hospital.
Well except for the general surgeons at the hospital who keep asking why we can't do them and are not fond of our consults for BKAs. .
It sounds as if the General Surgeons at your hospital don't want to do the BKAs. A lot of people consider it to be undesirable work. If you enjoy doing them then that's fine, but for a lot of doctors doing amps is similar to taking ER call -- not so much a privilege as it is a burden.
D
dyk343
Below the knee/tibial tuberosity.I understand the arguments for and against doing BKAs. I don't know, I just don't have an interest in doing any of that stuff.
I'll reiterate my prior comment in this thread, what happens when you get skin edge necrosis of the BKA stump you performed for your unsalvageable diabetic foot infection? Do you punt or do you keeping going and perform an AKA because the surgical issue "originated from the foot"?
Where does it end?
D
dyk343
It sounds as if the General Surgeons at your hospital don't want to do the BKAs. A lot of people consider it to be undesirable work. If you enjoy doing them then that's fine, but for a lot of doctors doing amps is similar to taking ER call -- not so much a privilege as it is a burden.
Yeah not a lot of people like doing wound care or amputations. I am one of the few who likes limb salvage I suppose.
Below the knee/tibial tuberosity.
But then you are back to confusing everyone with scope. You can do a BKA but you can't nail a tibia. Theyll also be confused when they consult you on your TMA patient who is back in house or in the ED and you tell them you can't do anything because the patient needs an AKA (according to vascular). You want to muddle the scope, making it harder on referring/consulting physicians so you can do one more procedure and manage the complications that come with it? You are insane...and I mean that in the nicest way possible.
And if for some crazy reason you are suggesting we be able to do anything below the knee (I don't think you are), then I hope you have to be the first to tell an orthopaedic surgeon we'd like to fix plateau fxs.
Advertisement - Members don't see this ad
D
dyk343
Within 50 years I would make a bold statement that our profession has osseous work to the tibial tuberosity. We have soft tissue to that level...But then you are back to confusing everyone with scope. You can do a BKA but you can't nail a tibia. Theyll also be confused when they consult you on your TMA patient who is back in house or in the ED and you tell them you can't do anything because the patient needs an AKA (according to vascular). You want to muddle the scope, making it harder on referring/consulting physicians so you can do one more procedure and manage the complications that come with it? You are insane...and I mean that in the nicest way possible.
And if for some crazy reason you are suggesting we be able to do anything below the knee (I don't think you are), then I hope you have to be the first to tell an orthopaedic surgeon we'd like to fix plateau fxs.
We've been doing BKAs for millennia. Overall, they really aren't that complicated of procedures, even family practitioners and GPs used to do them back in the day (50s). I really don't see why a competent podiatric surgeon that focuses on everything below the knee couldn't remove a limb below the knee, it really doesn't make sense.
Yeah not a lot of people like doing wound care or amputations. I am one of the few who likes limb salvage I suppose.
I'm thankful we have people like you around who enjoy that part of our job -- seriously.
I'll reiterate my prior comment in this thread, what happens when you get skin edge necrosis of the BKA stump you performed for your unsalvageable diabetic foot infection? Do you punt or do you keeping going and perform an AKA because the surgical issue "originated from the foot"?
Where does it end?
That line of logic would invalidate all podiatric surgical procedures, and especially amputations of the foot. If you take a toe and it doesn't heal, what's next? Transmetatarsal. Doesn't heal, what's next? Lisfranc. Doesn't heal, what's next? Chopart. Doesn't heal, what's next? Symes. Doesn't heal, what's next? Transtibial. Doesn't heal, what's next? Knee disarticulation. Etc etc all the way until you've got podiatrists amputating at the cervical level to save the head. With that line of logic podiatrists should not be allowed to perform any amputations. Heck, why should they even be allowed to touch the foot at all?
The OPs reasoning seems much more sound. In the near future the nationwide podiatric scope (if such a thing could ever be said to exist) could reasonably expand to include the leg in its entirety up to the tibial tubercle or thereabouts. If the disease, necrosis, or whatever continues then the patient could be passed of to another surgeon for a knee disarticulation or a transfemoral amputation, just like now you would pass it off for a transtibial.
The scope has changed a lot in the past 50 years and is sure to change more in the next 50. And so maybe you weren't trained to do transtibial amputations and you have no desire to, but that doesn't mean that the next generation of pods won't want/earn privileges up to the knee and that the generation after that won't want/earn privileges for the lower extremity in its entirety (can't imagine it reasonably extending beyond the hip articulation). You don't personally have to take part one way or the other, but for those who are trying to better themselves, better the field, and improve patient care (as the OP is), the least you could do is not get in the way of progress or try to talk them down.
#JustSayin
So let me get this straight? You became a podiatrist to take care of the foot and ankle? But that isn't enough so you want to do BKAs? Fine. But that isn't enough so you want to continue up until the hip joint? I guess my question is why dont you become an orthopedic surgeon? They can do take care of the lower extremity from the foot to the hip? Why are you reinventing the wheel. A podiatrist does foot and ankle. An orthopedist does MSK foot and ankle and MSK everywhere else.
I dont buy the line of reasoning that because a problem originiated in the foot and ankle, it automatically means a podiatrist takes care of it. Diabetes originates in the pancreas. Hepatobiliary surgeons do not care for diabetes patients. Melanoma that originates in the foot? Podiatrists dont give chemo/radiation for melanoma. Septic shock originates in the foot? Podiatrists dont manage the septic shock.
I dont buy the line of reasoning that because a problem originiated in the foot and ankle, it automatically means a podiatrist takes care of it. Diabetes originates in the pancreas. Hepatobiliary surgeons do not care for diabetes patients. Melanoma that originates in the foot? Podiatrists dont give chemo/radiation for melanoma. Septic shock originates in the foot? Podiatrists dont manage the septic shock.
So let me get this straight? You became a podiatrist to take care of the foot and ankle? But that isn't enough so you want to do BKAs? Fine. But that isn't enough so you want to continue up until the hip joint? I guess my question is why dont you become an orthopedic surgeon?
By your logic, why would anybody ever become a podiatrist then? You do realize that there's more to podiatry than the musculoskeletal system, don't you?
Y'all are blowing out of proportion the OP's mention of the problem originating in the foot/ankle. Obviously they meant that the podiatrist is a foot/ankle/lower extremity specialist who is well trained in the anatomy and physiology of the entire lower extremity as well as in orthopedic surgical techniques. Podiatric scope ranges from foot only in some states up to surgical treatments up to the knee or treatments of soft tissue up to the hip in others. If a podiatrist (like OP) has scrubbed in on multiple BKAs then they are as well trained as many (also better trained than many) to perform BKAs.
Here is the data to back up my point:
(1) An orthopedist can technically make it through an orthopedic residency by performing ZERO amputations, as it is not in their case log minimum number requirements.
https://www.acgme.org/acgmeweb/Port...esources/260_ORS_Case_Log_Minimum_Numbers.pdf
(2) The average orthopedist upon completion of residency has performed on average a whopping THREE femur/knee amputations and about SIX leg/ankle amputations.
https://www.acgme.org/acgmeweb/Portals/0/OrthopaedicSurgery_National_Report_Program_Version.pdf
But let's not question their training on the matter, because they have an MD behind their name...
Many years ago people would have scoffed at the idea of chiropractors treating anything but the spine (you know, since that's what their whole deal is made up around) but today they can treat pretty much the whole musculoskeletal system non-surgically as well as write some prescriptions. Many years ago people would have scoffed at osteopaths for talking about parity and wanting to do more than just put their hands on people (which since that can apparently treat everything, why would they need anything else...hmmm...) but here they are today with the exact same scope as MDs. I don't think any podiatrist is asking to treat systemic diseases, whether they have manifestations in the lower extremity or not. They are just looking to perform at the top of their scope and within the realm of their education, training, and experience (just like every other physician). The idea of performing BKAs within the next 10-15 years (OP's general idea), or slowly expanding the education and training to encompass surgical procedures up to the hip within the next 50 years (my idea I suppose) is not at all far fetched.
If you want to take care of MSK issues up to hip, become an orthopedic surgeon. If you want to take care of foot and ankle and only foot and ankle then become a podiatrist because thats what a podiatrist is, by definition. Its like saying that vet should take care of people because they use similar medicines and techniques. Its simply a matter of why reinvent the wheel. Go to medical school become an orthopedic surgeon and be, at the very least, an MSK LE specialist, and perform all the BKAs your heart desires, along with AKAs, along with hip and knee replacements. Or become a vascular surgeon or a general surgeon or whatever specialty it is that you want to practice, but dont go inventing some sort of scope for podiatrists because you do not want to go medical school.
I scrubbed in on a a bunch of surgeries in medical school and residency in other fields, and I wont perform them because I am not a (fill in the blank) specialist and if i wanted to do that type of surgery I should have specialized in the (fill in the blank)
I scrubbed in on a a bunch of surgeries in medical school and residency in other fields, and I wont perform them because I am not a (fill in the blank) specialist and if i wanted to do that type of surgery I should have specialized in the (fill in the blank)
I'm not seeing you present any cogent arguments. And anyway, at least where the OP is located, the orthopedists and vascular docs are not performing the procedures and that is the reason for this whole thread. If there is a niche that is not being filled, then there is cause for a related field (podiatry) to step in. And I mean actually related, not like vets *smh*.If you want to take care of MSK issues up to hip, become an orthopedic surgeon.
I'm not saying that today's podiatrists should be able to perform surgically up to the hip. Nor am I saying that the next generation of podiatrists should be able to. But don't act like such an idea is an abomination. In the past twenty years or so podiatry has gone from foot experts who maybe had a one year residency and maybe could perform some forefoot surgeries to foot/ankle/leg (i.e., anatomical leg, below knee) experts who are trained surgically (and medically) for the foot/ankle/leg. Three year residencies are now standard and some four year residencies are available. With this trend, what I am saying is that it wouldn't be unreasonable for the residency standards to be raised to four years across the board within the next 20 years. And if in five years of residency a general surgeon could adequately learn surgical procedures of the whole body or an orthopedic surgeon could adequately learn orthopedic procedures of the whole body then surely in four years a podiatric surgeon should be able to adequately learn surgical procedures of the entire lower extremity. If there were a trend in that direction then within the next 50 years podiatric surgeons could well practice up to the hip. My only point is that podiatrists, like any other physician, should be able to practice to the extent of their education and training. Surgically, up to the hip, the education and training is not there yet. Nobody is saying that it is. For newer podiatrists, up to the tibial tubercle (which could include transtibial amputations), there are certainly grounds to argue for that.
If a procedure is reasonably within the scope of the education and training of a physician, then it should reasonably be within their scope of practice. Those are the grounds for which you or anybody else argues that an MD is competent. Why should that logic not apply in this situation? IF the OP feels that they are adequately educated about the leg and they have scrubbed in on at least as many transtibial amputations as the average residency trained orthopedist, then why should they not be allowed to perform the procedure? You're getting too hung up on the name of a specialty and not looking at the actual education or training that may be going on or may go on in the future within that specialty, let alone the needs of the patients. And isn't that what medicine is really all about...tsk-tsk...
Podiatry has way too much work to do in the area of getting better applicants and providing better residency training across the board (the gap between the "best" programs and the "worst" programs is frightening), to be wasting time worrying about BKAs.
No doubt.Podiatry has way too much work to do in the area of getting better applicants and providing better residency training across the board (the gap between the "best" programs and the "worst" programs is frightening), to be wasting time worrying about BKAs.
Advertisement - Members don't see this ad
I dont know anything about you or what you want professionally in life. But if you want to operate up to the hip, and you want to do amps, and limb salvage or trauma work and joint replacement, I highly urge you to go to medical school to become a vascular surgeon or orthopedic surgeon. Whether you think its fair or not or right vs wrong, in your podiatry career you will never (or at least the chance is so tiny) get to do fem pop bypasses or stents or joints or bka/aka regardless of what that pathology is doing to the foot, and I mean actually do them (not scrub as a med student or intern), so if thats really what you want professionally then I seriously urge you to go to medical school. If you want to be a foot and ankle doc in some states and foot doc in others and only that, then go become a podiatrist and you will have a rewarding career, im sure. But dont go into podiatry (or any field) and think that you will change it to fit what you want to do in life.
At least thats a risk I wouldnt want to take with my career
At least thats a risk I wouldnt want to take with my career
I'm not saying that today's podiatrists should be able to perform surgically up to the hip. Nor am I saying that the next generation of podiatrists should be able to.
I realize that the podiatric scope expanding nationally to the knee is a longshot, let alone the hip. I'm being open minded and saying "who knows what will happen in the future?". I'm just positing a possibility. There are many podiatrists constantly pushing the limits of the scope just like every other health profession (NP, PA, PT, Chiro, etc.) and starting from the foot there aren't too many directions for expansion to choose from. I was trying to be reasonable though and so gave a timeline of fifty years, which is a freakin' long time and I'm sure I'll be long retired by then. I'll personally be perfectly content with the foot/ankle. But, like I said, who knows what the next generation and the generation after that will want or strive for—a generation being about 25 years of course.
I'll tell you what Grizz11, meet me here 50 years from today, then we'll discuss this further. If the podiatric scope hasn't expanded to the hip by then I'll buy you a beer. If it has, I'll let you buy me two 😉
But if you want to operate up to the hip, and you want to do amps, and limb salvage or trauma work and joint replacement
While I agree with your general premise (that our scope should only be within the foot, ankle, and the inferior tibiofibular joint - and not the hip), amputation, limb salvage, joint arthroplasty, and trauma are still important aspects of the specialty that podiatrists do indeed manage within that scope. It's important especially where the diabetic population is concerned. There's a "true stories from podiatric residency" thread on this subforum somewhere (EDIT: Found it! http://forums.studentdoctor.net/threads/true-stories-from-podiatric-residency.409888/), I would suggest taking a look at that and you'll definitely find trauma, amps, joint arthroplasty and arthrodesis, and limb salvage mentioned in there. Even TARs.
I can't figure out where you are practicing (you implied that you were out of residency?), but I can tell you that this mentality of "podiatrists can only perform conservative F&A care" is largely limited to online premed/doctor-related forums like SDN, and probably in the area you practice in (I'm betting northeast).
If you want to be a foot and ankle doc in some states and foot doc in others and only that, then go become a podiatrist and you will have a rewarding career, im sure.
Here are a list of states that include ankle within their scope of practice for podiatrists, in case you're curious:
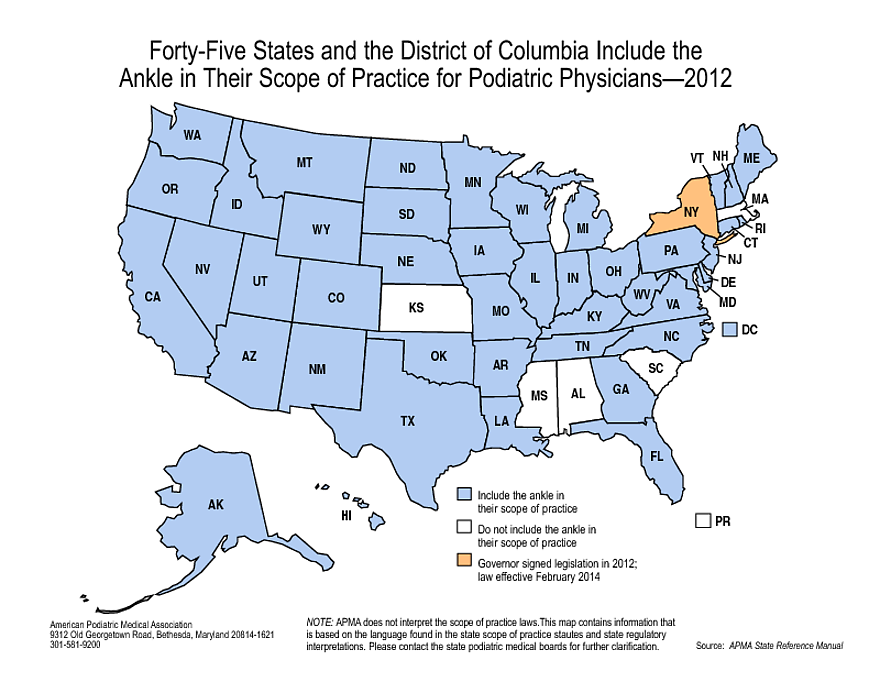
So honestly, it's only just those five states that still don't include ankle in their scope, but I'm willing to bet this will change in the near future.
Last edited:
D
dyk343
When did I ever say I wanted to operate to the level of the hip?
I don't think there is a gray area. You are able to put a nail (through the calc) in a tibia, take BMA and bone from the tibia, place a ring fixator, etc (and who fixes proximal fibula fxs?) as they relate and are needed to surgically correct pathology where the foot or ankle are involved.
You can't throw a tibial nail or ORIF a tibia for a shaft fx, for the same reason you can't perform a BKA. I mean sure, neither are too difficult from a technical standpoint for a pod with good training to perform. But you have to expand the scope across the board to include any and all pathology to below the knee. If you say "well we aren't asking to fix the tibia in trauma situations, just let us do BKAs" then you are right back to the whole lack of understanding of what a Podiatrist can or can't do.
Here's a funny story which Ankle Breaker already alluded to: in orientation for our new residents, a FP resident asked one of our interns who we had write prescriptions for our patients and who we sent them to for surgery...they will learn very quickly at our program that absolutely any pathology that relates to the foot or ankle is handled by our service at the hospital, and that we are the foot and ankle service within the ortho dept (and we even have a good size ortho residency program at our hospital). But the fact remains that they had literally no idea of our training or scope of practice.
Did I mention that I have no desire to do more pus than is already in our scope?
Yeah, when your BKAs fail, then you have to consult ortho for an AK anyway...eff that.
I enjoy limb salvage and reconstruction and I do think it would be beneficial for our scope to include the ability to do a BKA. Gen surg, ortho, and vascular surgery at my program all have asked (attendings and residents) why our service can't do them when we technically can do all the parts (at least in my state), just not the procedure as a whole.
So what if it becomes "consult ortho/vascular for an AKA". We already say to consult for a BKA. I think that sounds better and has a more definitive level of scope of practice as opposed to ... "well, we did the TMA, the next viable option is a BKA, ask someone else". Just my two cents.
So what if it becomes "consult ortho/vascular for an AKA". We already say to consult for a BKA. I think that sounds better and has a more definitive level of scope of practice as opposed to ... "well, we did the TMA, the next viable option is a BKA, ask someone else". Just my two cents.