Among the changes was an increase from 60 to 90 minutes in the time therapists have to conduct an initial assessment of children. Kaiser Permanente also committed to increase staffing, according to the union.
The vote marks the end of the longest mental health worker strike in American history.

www.sfgate.com
Therapists at Kaiser Permanente in Northern California voted Thursday to ratify a new contract with the health care giant, marking the end of the
longest strike by mental health workers in American history.
Workers voted 1,561 to 36 to end the 10-week strike and accept the contract. The vote came two days after a
tentative agreement was announced in a joint statement between Kaiser and the National Union of Healthcare Workers, which represents the 2,000 non-psychiatrist therapists of the HMO's Northern California branch. The four-year contract will be retroactive to September 2021, expiring in September 2025.
Key terms of the deal include an increase in pay for bilingual therapists; additional hours per week for all clinicians to “perform critical patient care duties,” such as responding to calls and emails and planning treatment; and commitments from Kaiser to hire more therapists and expand crisis services for patients.
Natalie Rogers, a Kaiser emergency mental health therapist in Santa Rosa, told SFGATE that ratifying the agreement means getting to help patients again, but acknowledges that the strike took a toll on patients and workers.
"It was important for us to go on strike, because we know that our patients deserve better care. ... But it came at a very high cost for a lot of therapists and their families and our patients not being able to receive care," she said. "That was the hardest part is that we were out for our patients, but they were also being hurt by us being out. So ratification really means that we are able to get back to work; we're able to work with Kaiser to continue to improve the mental health resources for our patients."
A key provision of the agreements is the introduction of five committees, which will meet over the span of six months and make recommendations for improvements to Kaiser's care model, which the insurer will be required to fund and implement. In its statement, the union said these committees are key to ensuring Kaiser will finally adhere to a state law that requires patients be scheduled for follow-up sessions within 10 business days of seeing a therapist, unless otherwise approved by a clinician.
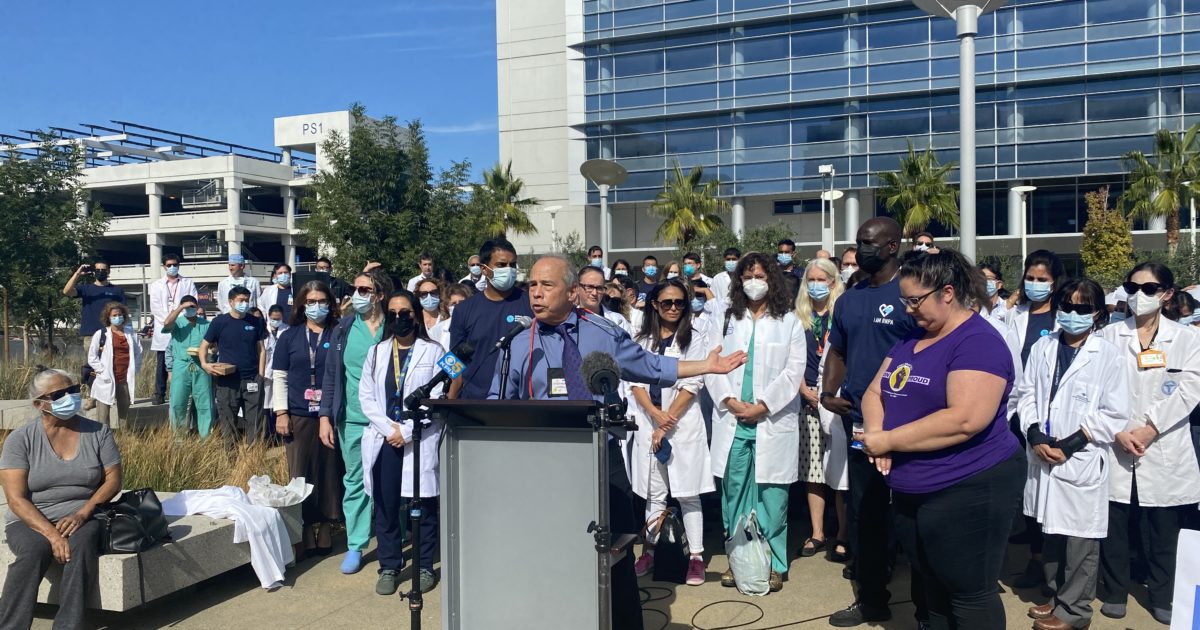
“I’m proud of Kaiser therapists for standing up for their patients and their profession,” Sal Rosselli, president of the National Union of Healthcare Workers, said in a statement provided by the union.
But the fight in Northern California — and elsewhere — continues. In
Hawaii, mental health care professionals have entered their eighth week of striking for similar demands.
"I just feel like there's still so much work to be done," Rogers said. "Us returning to work, we did so with a lot of compromise. And ultimately, we're not where we want to be as far as the care that we want to give to our patients, but it is a step in the right direction."
A representative for Kaiser did not immediately respond to a request for comment from SFGATE.