So with all the NPs and PAs being released into the workforce, how will family medicine shape up in the next 10 years? Are we looking at horrendous paycuts or will salary go up due to baby boomers?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Future of Fam Med- How will NPs and PA affect salary?
- Thread starter alisepeep
- Start date

- Joined
- Jun 26, 2001
- Messages
- 723
- Reaction score
- 294
Considering that the majority of PA's actually go into specialities, this is a medicine/surgery problem not a "family med" problem.
I know of a psych NP who has their own practice (no MD involved), I know of ER's staffed ONLY by PA's (no MD's on site). I know of suboxone/addiction clinics run ONLY by PA's. I know of women health clinics that ONLY have NPs. CRNA's, which are nurses, have won independence in many states.
How long will it be before a "cardiologist" NP sets up their own practice? or a "derm" NP? How long will it take before NP's start trying to become Primary surgeon?
All fields will continue to have trouble with midlevels, not just family medicine.
I know of a psych NP who has their own practice (no MD involved), I know of ER's staffed ONLY by PA's (no MD's on site). I know of suboxone/addiction clinics run ONLY by PA's. I know of women health clinics that ONLY have NPs. CRNA's, which are nurses, have won independence in many states.
How long will it be before a "cardiologist" NP sets up their own practice? or a "derm" NP? How long will it take before NP's start trying to become Primary surgeon?
All fields will continue to have trouble with midlevels, not just family medicine.
- Joined
- Apr 16, 2003
- Messages
- 805
- Reaction score
- 14
I have noticed an INCREASE in salary due to our clinic having midlevels. They generate RVU's and allow us to carry a larger patient panel. Patients are happy with the ability to get in fairly quickly with the midlevels for acute things if they cannot see their PCP. We cap the ratio of midlevels to physician in clinics (for supervisory purposes etc) so no risk to me of losing my job to them any time soon.
- Joined
- Mar 24, 2010
- Messages
- 4,074
- Reaction score
- 5,188
I have noticed an INCREASE in salary due to our clinic having midlevels. They generate RVU's and allow us to carry a larger patient panel. Patients are happy with the ability to get in fairly quickly with the midlevels for acute things if they cannot see their PCP. We cap the ratio of midlevels to physician in clinics (for supervisory purposes etc) so no risk to me of losing my job to them any time soon.
This has been my observation at the Family Med practices I've worked with too.
- Joined
- May 6, 2006
- Messages
- 269
- Reaction score
- 1
Considering that the majority of PA's actually go into specialities, this is a medicine/surgery problem not a "family med" problem.
And then I just read an article by an NP saying they go mostly into primary care...so who is to be believed?
I say the reality is they will go to whatever pays them the most that happens to be available at a given moment
How long will it be before a "cardiologist" NP sets up their own practice? or a "derm" NP? How long will it take before NP's start trying to become Primary surgeon?
All fields will continue to have trouble with midlevels, not just family medicine.
All of them for sure, but currently FM more than others.
I have noticed an INCREASE in salary due to our clinic having midlevels. They generate RVU's and allow us to carry a larger patient panel. Patients are happy with the ability to get in fairly quickly with the midlevels for acute things if they cannot see their PCP.
Most probable it won't be long before a majority of patients won't care who sees them as long as they think they are receiving "adequate" care, waiting less, and paying less.
We cap the ratio of midlevels to physician in clinics (for supervisory purposes etc) so no risk to me of losing my job to them any time soon.
That is no guarantee whatsoever for job security...
Who knows how the landscape of medicine in the US is going to change in a few years with more midlevels pushing for independence and we gladly allowing it.
- Joined
- Jun 26, 2001
- Messages
- 723
- Reaction score
- 294
And then I just read an article by an NP saying they go mostly into primary care...so who is to be believed?
I say the reality is they will go to whatever pays them the most that happens to be available at a given moment
Although the percentage of PA/NPs may be majority in primary care at the movement- look at PA/NP's placements for the past few years, speciality placements are overwhelming. They ARE going where the money is, for example: ER often pays PA's >20-30$/hr more than a family medicine is able to!
D
deleted87716
Only 1/4 of PAs are in primary care. The rest are in other fields. So, it's not an "FM problem."
Source: http://img.medscape.com/news/2014/ih_140811_pie_chart_specialties_800x600.jpg
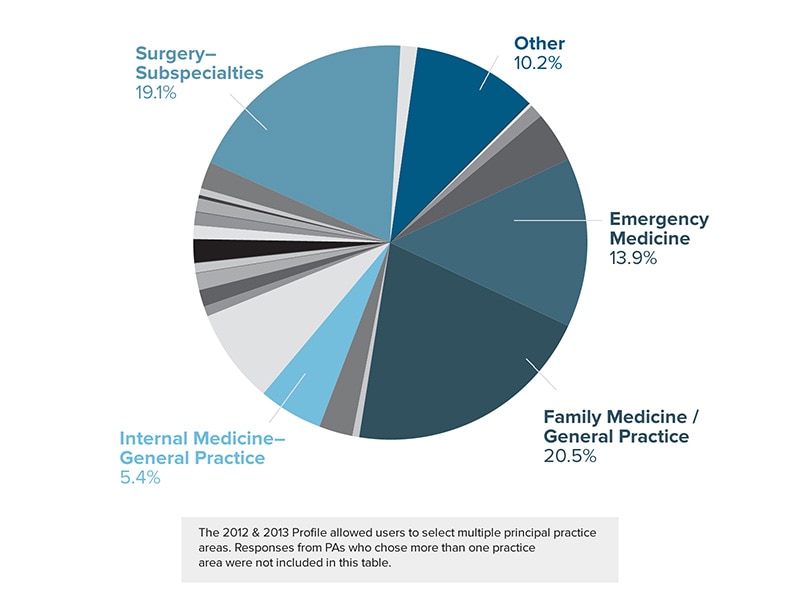
In fact, despite the increase in the number of non-physician providers, more and more of them are going into non-primary care specialties.
Source: http://www.ruralmedicaleducation.org/basichealthaccess/Too_Many_Specialists.htm

Source: http://img.medscape.com/news/2014/ih_140811_pie_chart_specialties_800x600.jpg
In fact, despite the increase in the number of non-physician providers, more and more of them are going into non-primary care specialties.
Source: http://www.ruralmedicaleducation.org/basichealthaccess/Too_Many_Specialists.htm
Last edited by a moderator:
- Joined
- Jun 26, 2001
- Messages
- 723
- Reaction score
- 294
Much to the government's surprise, PA/NPs follow the money as opposed to going to areas where no doctors want to go, or working low pay jobs with complicated patients.
The government solution: make more PA/NPs schools and give them a wider scope of practice... Will result in PA/NPs filling subspecialities and making even more money and still have the exact same primary care gap.
The government solution: make more PA/NPs schools and give them a wider scope of practice... Will result in PA/NPs filling subspecialities and making even more money and still have the exact same primary care gap.
- Joined
- May 6, 2006
- Messages
- 269
- Reaction score
- 1
I'm sure if you ask the NP whose article I quoted she will also give you all kind of numbers and cute graphical pies and whatnot too to support her claim that most NPs go into primary care...
I'll tell you what I see in my city. Most outpatient FM/IM employers hire midlevels and one (non-residential) physician to serve as medical director.
For many (if not most) of offices they're not even hiring FM docs. The moment they pay one offsite FM doc, a fee to be medical director they have midlevels do all the medical care.
They [employers] in FM and other areas of practice, are heavily pushing (e.i. controlled rx rights for midlevels) so that they do not have to pay a doc.
If it wasn't because of current state licensing regulation everybody and their mother would pay only midlevels to see patients...and many patients (if not most) of course will think they're seeing a doc when the office sets them up with a midlevel.
Where does that leave job security for a physician?
Let's see how things will look in a few years, but following the money trace one would think things might not be too rosey for physician in the future.
I'll tell you what I see in my city. Most outpatient FM/IM employers hire midlevels and one (non-residential) physician to serve as medical director.
For many (if not most) of offices they're not even hiring FM docs. The moment they pay one offsite FM doc, a fee to be medical director they have midlevels do all the medical care.
They [employers] in FM and other areas of practice, are heavily pushing (e.i. controlled rx rights for midlevels) so that they do not have to pay a doc.
If it wasn't because of current state licensing regulation everybody and their mother would pay only midlevels to see patients...and many patients (if not most) of course will think they're seeing a doc when the office sets them up with a midlevel.
Where does that leave job security for a physician?
Let's see how things will look in a few years, but following the money trace one would think things might not be too rosey for physician in the future.
- Joined
- Apr 22, 2006
- Messages
- 2,857
- Reaction score
- 2,798
Where are you located? I have never seen a private practice PCP office that was mostly midlevels. Around my area, the private practice (AKA those with insurance) population KNOW if their provider is a MD or midlevel. They would not tolerate having a NP primary care provider.I'm sure if you ask the NP whose article I quoted she will also give you all kind of numbers and cute graphical pies and whatnot too to support her claim that most NPs go into primary care...
I'll tell you what I see in my city. Most outpatient FM/IM employers hire midlevels and one (non-residential) physician to serve as medical director.
For many (if not most) of offices they're not even hiring FM docs. The moment they pay one offsite FM doc, a fee to be medical director they have midlevels do all the medical care.
They [employers] in FM and other areas of practice, are heavily pushing (e.i. controlled rx rights for midlevels) so that they do not have to pay a doc.
If it wasn't because of current state licensing regulation everybody and their mother would pay only midlevels to see patients...and many patients (if not most) of course will think they're seeing a doc when the office sets them up with a midlevel.
Where does that leave job security for a physician?
Let's see how things will look in a few years, but following the money trace one would think things might not be too rosey for physician in the future.
- Joined
- May 6, 2006
- Messages
- 269
- Reaction score
- 1
Where are you located? I have never seen a private practice PCP office that was mostly midlevels. Around my area, the private practice (AKA those with insurance) population KNOW if their provider is a MD or midlevel. They would not tolerate having a NP primary care provider.
MIA
D
deleted87716
I'm sure if you ask the NP whose article I quoted she will also give you all kind of numbers and cute graphical pies and whatnot too to support her claim that most NPs go into primary care...
I doubt it. She's probably just parroting what she's been told by other NPs. Repeating a falsehood doesn't make it true, regardless of how many times you repeat it.
D
deleted87716
- Joined
- Apr 4, 2009
- Messages
- 17,237
- Reaction score
- 13,034
Funny they tell legislators they're the solution to primary care.Only 1/4 of PAs are in FM. The rest are in other fields. So, it's not an "FM problem."
Source: http://www.pg2pa.org/DITL/index.html

In fact, despite the increase in the number of non-physician providers, more and more of them are going into non-primary care specialties.
Source: http://www.ruralmedicaleducation.org/basichealthaccess/Too_Many_Specialists.htm
- Joined
- Jan 9, 2006
- Messages
- 15,396
- Reaction score
- 7,734
Miami is quite different from the rest of the country; it's not even quite the same as other parts of Florida. That's like extrapolating your entire understanding of the US by spending all of your time in NYC or SF.
- Joined
- Jan 9, 2006
- Messages
- 15,396
- Reaction score
- 7,734
Is that anywhere near BFE? 😉
About 3 hours south of BFE. 😛
As a (marginally related) aside, this is the BEST twitter feed. Highly entertaining:
https://twitter.com/_FloridaMan
- Joined
- Mar 13, 2012
- Messages
- 636
- Reaction score
- 660
While this is certainly the dream of corp-med, there are a few shining lights.
1) people want to see a doctor. A few patients may not notice, but overwhelmingly patients know that they haven't seen a physician. If it's just a sinus infection they don't care, but when their chronic condition isn't improving as they hoped they are going to question the quality of medical advice they are receiving. It is a natural response.
2) All this hoopla about NPs doing independent practice is predicated upon the assumption that they actually want to do primary care medicine. Most evidence, and personal experience, would indicate otherwise. The money is in specialist care, that's why you always see NP/PAs in a derm office or a cardiology group. If money is already tight in FM for physicians, then why do you think an NP, who currently gets reimbursed 85% of the doctors rate by CMS, will magically be able to make money? They won't, and they don't. NP/PA's don't want primary care.
3) Lastly, if any NP/PA does want to enter FM I would gladly stand side by side with them if it means turning around the way we focus on speciality medicine vs primary care, intervention vs prevention. I see any " encroachment" by an NP into FM as an opportunity to widen our political pull, because currently there is very little "encroachment" coming from the medical school down the road.
1) people want to see a doctor. A few patients may not notice, but overwhelmingly patients know that they haven't seen a physician. If it's just a sinus infection they don't care, but when their chronic condition isn't improving as they hoped they are going to question the quality of medical advice they are receiving. It is a natural response.
2) All this hoopla about NPs doing independent practice is predicated upon the assumption that they actually want to do primary care medicine. Most evidence, and personal experience, would indicate otherwise. The money is in specialist care, that's why you always see NP/PAs in a derm office or a cardiology group. If money is already tight in FM for physicians, then why do you think an NP, who currently gets reimbursed 85% of the doctors rate by CMS, will magically be able to make money? They won't, and they don't. NP/PA's don't want primary care.
3) Lastly, if any NP/PA does want to enter FM I would gladly stand side by side with them if it means turning around the way we focus on speciality medicine vs primary care, intervention vs prevention. I see any " encroachment" by an NP into FM as an opportunity to widen our political pull, because currently there is very little "encroachment" coming from the medical school down the road.
- Joined
- May 6, 2006
- Messages
- 269
- Reaction score
- 1
Miami is quite different from the rest of the country; it's not even quite the same as other parts of Florida. That's like extrapolating your entire understanding of the US by spending all of your time in NYC or SF.
Forget generic city differences
Forget outlier communities
And forget "current" points of comparison
It's not about how things are now in other metro areas
The point is the trend...how will things be in the future?
Why can't what's happening here be a reflection of how things will turn out in the future in other metro US areas?
The same economic/social forces that make the medical practice environment here could very well be growing in your metro area
I think those who focus only on how things look now around you, data, statistics etc are deluded
Look at the trends...you want to look at numbers? Look at the craploads of midlevels being churned out
What's going to happen when there's more midlevels than speciality work openings available, where will they go practice then?
Do you still think they will not seek primary care jobs if only those are available?
Couple that with their increasing push for independent practice plus the challenge to have the average person know who is really a doc
And as if that wasn't enough add economic incentives (e.i. lower cost) for people to care less whether they're seen by a midlevel practicing independently
So this isn't an FM only problem? Maybe, but FM is what we're discussing here
Save this post for posterity...
- Joined
- Sep 26, 2009
- Messages
- 2,854
- Reaction score
- 815
That is the future of FM when Walmart is planning to have walk-in clinics all over the US and staff them with NPs... They will charge $40/visit to see your (the) doctor who happen to be a nurse practitioner...
http://www.forbes.com/sites/dandiam...ls-new-primary-care-clinics/?partner=yahootix
http://www.forbes.com/sites/dandiam...ls-new-primary-care-clinics/?partner=yahootix
D
deleted87716
That is the future of FM when Walmart is planning to have walk-in clinics all over the US and staff them with NPs... They will charge $40/visit to see your (the) doctor who happen to be a nurse practitioner...
http://www.forbes.com/sites/dandiam...ls-new-primary-care-clinics/?partner=yahootix
In-store clinics are nothing new. They've been the "next big thing" for years now, yet most are still trying to figure out how to stay profitable once cold and flu season passes and they can't continue handing out unnecessary Zithromax prescriptions.
The reality is that most of these clinics are ill-prepared to manage chronic medical conditions. Let 'em try.
Last edited by a moderator:
- Joined
- Jan 25, 2013
- Messages
- 274
- Reaction score
- 93
Considering that the majority of PA's actually go into specialities, this is a medicine/surgery problem not a "family med" problem.
I know of a psych NP who has their own practice (no MD involved), I know of ER's staffed ONLY by PA's (no MD's on site). I know of suboxone/addiction clinics run ONLY by PA's. I know of women health clinics that ONLY have NPs. CRNA's, which are nurses, have won independence in many states.
How long will it be before a "cardiologist" NP sets up their own practice? or a "derm" NP? How long will it take before NP's start trying to become Primary surgeon?
All fields will continue to have trouble with midlevels, not just family medicine.
Nephrology NP/PA are coming to a dialysis clinic near you.
- Joined
- Aug 10, 2014
- Messages
- 22
- Reaction score
- 8
While this is certainly the dream of corp-med, there are a few shining lights.
1) people want to see a doctor. A few patients may not notice, but overwhelmingly patients know that they haven't seen a physician. If it's just a sinus infection they don't care, but when their chronic condition isn't improving as they hoped they are going to question the quality of medical advice they are receiving. It is a natural response.
2) All this hoopla about NPs doing independent practice is predicated upon the assumption that they actually want to do primary care medicine. Most evidence, and personal experience, would indicate otherwise. The money is in specialist care, that's why you always see NP/PAs in a derm office or a cardiology group. If money is already tight in FM for physicians, then why do you think an NP, who currently gets reimbursed 85% of the doctors rate by CMS, will magically be able to make money? They won't, and they don't. NP/PA's don't want primary care.
3) Lastly, if any NP/PA does want to enter FM I would gladly stand side by side with them if it means turning around the way we focus on speciality medicine vs primary care, intervention vs prevention. I see any " encroachment" by an NP into FM as an opportunity to widen our political pull, because currently there is very little "encroachment" coming from the medical school down the road.
I essentially agree with the above. People ultimately want to see the doctor and the vast majority of patients know a "doctor" from an assistant, be it a PA or NP.
1. When diseases are stable, like HTN, DM, COPD, CHF, etc I think it's ok to have an NP/PA see the patient every now and then or more often than the physician even. The patient will have more access to the system, it'll keep them out of the hospital, it will allow the doctor to see more active patients, etc. If the patient has a question the doctor can always go and talk to the patient.
2. I think NP/PAs can really help expand primary care. I do think doctors should oversee them and at least assess all new patients and see the "sicker" patients. One doctor with 4 midlevels can help way more people than one doctor alone.
3. I personally wouldn't be worried at all about midlevels "taking over" primary care. Midlevels don't like primary care for the same reason many doctors don't like it... it's pretty hard and doesn't pay all that well. It's much easier to see problem focused subspecialty patients because the scope is much smaller for midlevels and it's easy to pawn stuff back to the pcp. But as with all fields many things are missed by midlevels because they won't see subtleties or think outside their algorithmic knowledge base. It'll all work itself out eventually I think.
- Joined
- Aug 10, 2014
- Messages
- 22
- Reaction score
- 8
That is the future of FM when Walmart is planning to have walk-in clinics all over the US and staff them with NPs... They will charge $40/visit to see your (the) doctor who happen to be a nurse practitioner...
http://www.forbes.com/sites/dandiam...ls-new-primary-care-clinics/?partner=yahootix
I think this will effect EM more than FM. People aren't going to leave their doctor for a NP at walmart. The point of these clinics is to get poor people into walmart. I think there are both good and bad things about these clinics.
1. Good = more access to basic care (not "primary care") for poor people. If they have a stable illness a NP should be at least somewhat capable of handling it (how hard is it to prescribe hctz for example in an otherwise healthy 50 yo M). It will also increase compliance with health maintenance aspects of primary care which doesn't take medical school to learn. It will decrease ER utilization.
2. Bad = walmart calling it "primary care" diminishes what primary care doctors actually do. Some people may never seek out a physician if things aren't going well. The NP may not refer to a physician if things aren't going well. NPs have been shown that their primary care skills are poor and overall more expensive to the system.
So overall I don't think walmart will be successful. Unless people buy from their retail store the medical care aspect won't be profitable and walmart will close these clinics. And I think eventually laws will be passed limiting what NPs can do. Not sure when but it will come eventually.
- Joined
- Sep 26, 2009
- Messages
- 2,854
- Reaction score
- 815
Most (if not all) NP will disagree with that first highlighted statement and they will point out studies that say they have equal or better outcomes to the MD/DO... Not that I agree with them or these studies. They will also say that all the time physicians spend in med school is not needed to be a PCP.1. Good = more access to basic care (not "primary care") for poor people. If they have a stable illness a NP should be at least somewhat capable of handling it (how hard is it to prescribe hctz for example in an otherwise healthy 50 yo M). It will also increase compliance with health maintenance aspects of primary care which doesn't take medical school to learn. It will decrease ER utilization.
2. Bad = walmart calling it "primary care" diminishes what primary care doctors actually do. Some people may never seek out a physician if things aren't going well. The NP may not refer to a physician if things aren't going well. NPs have been shown that their primary care skills are poor and overall more expensive to the system.
So overall I don't think walmart will be successful. Unless people buy from their retail store the medical care aspect won't be profitable and walmart will close these clinics. And I think eventually laws will be passed limiting what NPs can do. Not sure when but it will come eventually.
Law will pass limiting what NPs can do? You are not serious with this statement! They are getting their scope expanded every day by state legislatures and you think these states will go back and limit what NPs can do... Maybe you should visit allnursesdotcom so you can see how these NPs think...they think now they should have some kind privilege to do 'minor' surgeries after 1 year of training... If you think they can take away the scope they have already given to these people, I really don't know what to tell you...
Last edited:
D
deleted6669
Why is everyone surprised when PAs/NPs follow docs into specialties? If primary care paid as well as surgery or dermatology or if there were an adequate # of loan repayment programs these folks would do primary care. I know MANY PAs/NPs who want to do primary care, look all over for loan repayment programs(NHSC and state programs accept a very limited # of folks), then end up taking jobs in fields like urology or rheumatology in which they have no interest just so they can pay their loans off. It's kind of a no brainer: 60 hrs/week in primary care for 80k vs 40 hrs/week for 90 k in any # of specialties as a new grad. I work in a rural/underserved setting not for the money(which is ok but less than I could make if I worked any generic HMO urgent care) , but for the scope of practice, respect, and autonomy.
I don't think you will see any new laws limiting NPs. Every year they gain a few more states for full independent practice. I think it is up to something like 22 now. PAs work under the medical board so physicians have the final say in our scope of practice and Physician to PA ratios. There are also vast differences between PA and NP training as most of you probably realize.
I don't think you will see any new laws limiting NPs. Every year they gain a few more states for full independent practice. I think it is up to something like 22 now. PAs work under the medical board so physicians have the final say in our scope of practice and Physician to PA ratios. There are also vast differences between PA and NP training as most of you probably realize.
D
deleted6669
From the Aug/Sept AARP magazine that goes to 20 gillion folks over 55:
http://www.aarp.org/health/healthy-living/info-2014/nurse-practitioners-fill-the-gap.html
http://www.aarp.org/health/healthy-living/info-2014/nurse-practitioners-fill-the-gap.html
- Joined
- Aug 10, 2014
- Messages
- 22
- Reaction score
- 8
Most (if not all) NP will disagree with that first highlighted statement and they will point out studies that say they have equal or better outcomes to the MD/DO... Not that I agree with them or these studies. They will also say that all the time physicians spend in med school is not needed to be a PCP.
Law will pass limiting what NPs can do? You are not serious with this statement! They are getting their scope expanded every day by state legislatures and you think these states will go back and limit what NPs can do... Maybe you should visit allnursesdotcom so you can see how these NPs think...they think now they should have some kind privilege to do 'minor' surgeries after 1 year of training... If you think they can take away the scope they have already given to these people, I really don't know what to tell you...
I'm sure you don't agree with the bolded part above being that you are in med school. But in case you do agree and want to be a super subspecialist and think primary care is easy take it from me and probably most people here that primary care is pretty challenging. Yeah sure there are plenty of "easy" cases in healthy people that don't really need medical school and residency training to care for... e.g. most health maintenance things, simple sinusitis, uncomplicated influenza, etc. But when you start having issues more vague and complicated in older/sicker patients, or difficult issues in seemingly younger healthy patients you'll be glad you had all that training. And when you are in residency and see patients in the hospital and also in clinic who recently saw an NP in clinic you'll see how ridiculously incomplete their training is. If anything NPs are more suited for helping subspecialists than primary care because subspecialists are, by definition, more focused.
In regards to laws, nurses can fight all they want but in the end they will get hit. In the short term laws may favor them but I don't see it happening in the long term.
- Joined
- Sep 26, 2009
- Messages
- 2,854
- Reaction score
- 815
I don't agree with it at all... I was pointing out how irrational these people can be.I'm sure you don't agree with the bolded part above being that you are in med school. But in case you do agree and want to be a super subspecialist and think primary care is easy take it from me and probably most people here that primary care is pretty challenging. Yeah sure there are plenty of "easy" cases in healthy people that don't really need medical school and residency training to care for... e.g. most health maintenance things, simple sinusitis, uncomplicated influenza, etc. But when you start having issues more vague and complicated in older/sicker patients, or difficult issues in seemingly younger healthy patients you'll be glad you had all that training. And when you are in residency and see patients in the hospital and also in clinic who recently saw an NP in clinic you'll see how ridiculously incomplete their training is. If anything NPs are more suited for helping subspecialists than primary care because subspecialists are, by definition, more focused.
In regards to laws, nurses can fight all they want but in the end they will get hit. In the short term laws may favor them but I don't see it happening in the long term.
Last edited:
- Joined
- May 6, 2006
- Messages
- 269
- Reaction score
- 1
So you thought NPs weren't interested in primary care?
Nurse practitioner opens concierge practice:
http://www.waaytv.com/news/decatur-...5c-2990-11e4-9d91-001a4bcf6878.html?success=1
Nurse practitioner opens concierge practice:
http://www.waaytv.com/news/decatur-...5c-2990-11e4-9d91-001a4bcf6878.html?success=1
D
deleted87716
So you thought NPs weren't interested in primary care?
Nurse practitioner opens concierge practice:
http://www.waaytv.com/news/decatur-...5c-2990-11e4-9d91-001a4bcf6878.html?success=1
Report back in a year.
- Joined
- May 6, 2006
- Messages
- 269
- Reaction score
- 1
Report back in a year.
Fair enough, let's see if in a year she has gone into something like derm lol
- Joined
- Jan 9, 2007
- Messages
- 244
- Reaction score
- 105
I completely agree that, if anything, NPs and PAs have helped family physicians INCREASE their revenue - especially at clinics that depend on high volume. While the public may not know the difference between MD/DO and PA/NP (and yes, there are quite a few PAs/NPs that fancy themselves as physicians), in my short experience as a practicing physician, I have seen that employers certainly know the difference. At my own clinic, by far the majority of missed diagnoses and dropped balls were by NPs (the PAs are fine actually) and not by the physicians, and this is reflected in the incident reports. I can't read the future, but my advice would be to have faith in your degree and in your education. I can assure you that don't regret becoming a family medicine doctor at all. (That said, I'll be sure to report back in 10 years 😉
- Joined
- Jan 20, 2016
- Messages
- 285
- Reaction score
- 551
It looks like they are still at it. Better join now so you too can have 24/7 access to a "practitioner" :Fair enough, let's see if in a year she has gone into something like derm lol
A Heartbeat Away... - HOME:
The movement to allow NPs to practice independently is scary as hell. There are a number of subpar online training programs cranking out thousands of new DNPs who then go on to lobby for full rights to practice as "doctors". No, a DNP who completed an online class is not as qualified as a board certified FM doc, but the people who write the laws allowing them to practice as doctors don't understand or care about that. We need to start organizing to fight this and pouring money into lobbying against the Noctors. If we don't, early career doctors WILL get screwed over.
I also strongly recommend refusing to train NP students or give curbside help to NPs. You're training your replacement if you do.
Last edited:
- Joined
- Nov 25, 2009
- Messages
- 140
- Reaction score
- 148
I'm heavily biased but if you're working for a hospital or paid by Medicare and the insurers, then you're a fungible commodity and can be replaced my midlevels as soon as they have enough of them.
Market your extra training directly to patients and work for them. I'm happy to have my bedside manner, degree and training compete with the midlevels' in that market.
Market your extra training directly to patients and work for them. I'm happy to have my bedside manner, degree and training compete with the midlevels' in that market.
Last edited:
D
deleted87716
If you're in private practice, the midlevels are working for you, "independent" or not. Plus, you're likely making money off them.
- Joined
- Mar 12, 2006
- Messages
- 226
- Reaction score
- 16
If you're in private practice, the midlevels are working for you, "independent" or not. Plus, you're likely making money off them.
A lot of $$$ "off them"
There's no true independent. It's a total BS.
- Joined
- Jan 20, 2016
- Messages
- 285
- Reaction score
- 551
I'm heavily biased but if your working for a hospital or paid by Medicare and the insurers, then you're a fungible commodity and can be replaced my midlevels as soon as they have enough of them.
Market your extra training directly to patients and work for them. I'm happy to have my bedside manner, degree and training compete with the midlevels' in that market.
We need to have PR campaigns to educate patients on how to tell if their "doctor" is an actual physician or a nurse with a DNP, because a lot of patients don't even know they're not seeing a real doctor.
If patients understand what's going on, I absolutely agree they will still choose a physician over a poorly trained nurse. However at the rate that NPs are being created and turned loose, I do fear that we are going to lose the PR battle when there are a ton of NPs telling people they have "the brain of a doctor and the heart of a nurse." I think it is completely possible that within my career we will see a situation where physicians are competing for a small market of wealthy patients who are savvy enough to see value in the training of a physician and have the means to go outside the system for care, while the majority of people get mediocre care from NPs using algorithms and cookbook medicine
- Joined
- Nov 25, 2009
- Messages
- 140
- Reaction score
- 148
A lot of $$$ "off them"
There's no true independent. It's a total BS.
If you're in private practice, the midlevels are working for you, "independent" or not. Plus, you're likely making money off them.
Actually, in a lot of states like Maine, NPs can be fully independent.
- Joined
- Nov 25, 2009
- Messages
- 140
- Reaction score
- 148
Thanks for pointing that out. I'll use that. I thought AAFP, like a broken clock that's right twice daily (The other time being its DPC support), briefly put out some material like this a couple of years ago but can't find it online this morning.
Last edited:
- Joined
- Jan 20, 2016
- Messages
- 285
- Reaction score
- 551
Yes, NPs are COMPLETELY INDEPENDENT (no physician oversight needed) in 22 states so far. They are working on becoming independent in the other states (I believe there are bills allowing them to be independent in TX and PA pending right now) :
AANP - State Practice Environment
We need to take this threat seriously if our profession is going to survive. Pretty soon, NPs will be able to function on the same level of physicians in every state and they will outnumber us. Pretty soon, people won't even remember that doctors used to be physicians because it will just be the norm to go see a DNP who calls him/herself "Doctor" for your care.
What is the AMA doing about this? What is your state medical society doing about it? To me, this should be the #1 priority for these organizations, because if we don't have a job or aren't making enough to pay back our student loans, there is no point to becoming a physician and none of the other issues on AMA's agenda matter at all.
AANP - State Practice Environment
We need to take this threat seriously if our profession is going to survive. Pretty soon, NPs will be able to function on the same level of physicians in every state and they will outnumber us. Pretty soon, people won't even remember that doctors used to be physicians because it will just be the norm to go see a DNP who calls him/herself "Doctor" for your care.
What is the AMA doing about this? What is your state medical society doing about it? To me, this should be the #1 priority for these organizations, because if we don't have a job or aren't making enough to pay back our student loans, there is no point to becoming a physician and none of the other issues on AMA's agenda matter at all.
Last edited:
D
deleted87716
Actually, in a lot of states like Maine, NPs can be fully independent.
The point is, most of them don't want to work completely on their own. They know their limitations, and it's just as difficult (if not moreso) for an NP to survive in solo or small practice as it is for a physician. I'm sure some are doing it, but they're in the minority.
D
deleted87716
What is your state medical society doing about it?
I could tell you, but then I'd have to kill you. 😉
D
deleted87716
Thanks for pointing that out. I'll use that. I thought AAFP, like a broken clock that's right twice daily (The other time being its DPC support), briefly put out some material like this a couple of years ago but can't find it online this morning.
They have some stuff here: http://www.aafp.org/advocacy/informed/workforce/scope.html
- Joined
- Dec 14, 2004
- Messages
- 506
- Reaction score
- 742
Reading this thread made me think of Baghdad Bob.
Pencil me in as being a bit worried as well. Sure the FNPs may not want primary care as they're going through school but it is a numbers game. More and more graduate every year, there are only so many specialist gigs to go around and there are plenty of family docs hiring, and those new grad FNPs have big loans and usually families as well. The job that I didn't really intend for sure pays a lot better than the one I don't have.
There is an FNP in town who practices derm independently. Is her training even close to a dermatologist? Not even close. Does it take 4 years of medical school and residency to handle cryo, simple biopsies, acne management, botox and low/medium potency topical steroid management? Lesion not responding, refer to dermatology. Pt none the wiser in most cases unfortunately.
Lawyers run the government and MBAs run hospital systems. Education/objectives for both focuses on the money. New FP grads are too busy trying to pay back their ungodly student loans to come up with an adequate bribe (I mean lobbying). In a decade, I fear things will look drastically different (like Marty McFly going back to 1955 different) than how they are today in primary care. We lose more autonomy every year. I hope I'm wrong.
Last edited:
- Joined
- Jul 28, 2004
- Messages
- 28,783
- Reaction score
- 61,866
Don't be worried. I get new patients all the time who come to my cash-only practice (with good insurance) who want to make sure they never get stuck seeing a midlevel.
- Joined
- Sep 16, 2016
- Messages
- 335
- Reaction score
- 402
Yes, NPs are COMPLETELY INDEPENDENT (no physician oversight needed) in 22 states so far. They are working on becoming independent in the other states (I believe there are bills allowing them to be independent in TX and PA pending right now) :
AANP - State Practice Environment
We need to take this threat seriously if our profession is going to survive. Pretty soon, NPs will be able to function on the same level of physicians in every state and they will outnumber us. Pretty soon, people won't even remember that doctors used to be physicians because it will just be the norm to go see a DNP who calls him/herself "Doctor" for your care.
What is the AMA doing about this? What is your state medical society doing about it? To me, this should be the #1 priority for these organizations, because if we don't have a job or aren't making enough to pay back our student loans, there is no point to becoming a physician and none of the other issues on AMA's agenda matter at all.
Melodramatic much?
- Joined
- Jan 20, 2016
- Messages
- 285
- Reaction score
- 551
Here is a video that the TX NP organization made to campaign for full practice rights in Texas:
Notice that the commercial is telling people that NPs provide the same level of care and have equal patient outcomes.
They don't want to work under you. They want to replace you. If you want to keep pretending this isn't happening until it's too late, well, then I guess our profession deserves what is about to happen to it.
Yes, you can say I am melodramatic, because this issue does work me up. However, I don't see anyone actually providing data to tell me why we shouldn't be worried about the fact that 20,000+ new NPs are graduating every year and that an increasing number of states are letting them do more and more without any physician oversight. Things aren't too bad yet - for now, there are still enough patients to go around that most docs can still find jobs easily - but to me it is clear things are heading in a direction that is very worrying. I think we all should be fighting this.
Notice that the commercial is telling people that NPs provide the same level of care and have equal patient outcomes.
They don't want to work under you. They want to replace you. If you want to keep pretending this isn't happening until it's too late, well, then I guess our profession deserves what is about to happen to it.
Yes, you can say I am melodramatic, because this issue does work me up. However, I don't see anyone actually providing data to tell me why we shouldn't be worried about the fact that 20,000+ new NPs are graduating every year and that an increasing number of states are letting them do more and more without any physician oversight. Things aren't too bad yet - for now, there are still enough patients to go around that most docs can still find jobs easily - but to me it is clear things are heading in a direction that is very worrying. I think we all should be fighting this.
Last edited:
Similar threads
- Replies
- 0
- Views
- 710
- Replies
- 0
- Views
- 2K