- Joined
- Feb 25, 2010
- Messages
- 4,263
- Reaction score
- 1,563
- Points
- 5,356
- Attending Physician

Im not certain how to stop prescribing but I would suggest to new grads not to start.
I never prescribed opioids when I started my practice. It was a tough go business-wise for the first several years but now it is a nonissue. I can't remember the last time I was even asked by a patient for a script
Is hydrocodone ok? Just the lesser of two evils?Very lucky. I actually wish we could just outlaw oxycodone - an oxycodone free pain clinic. I think that would take care of most of the issues. Its dilaudid IV in the hospital and oxycodone in the outpatient world.
Is hydrocodone ok? Just the lesser of two evils?
Anecdotally yes. 1:1 equivalence with morphine, I don’t seem to see the same drug craving from patients as I do oxycodone. I mean ideally no opioids but I think if we got rid of oxycodone it’s be great
The easiest way is to move to another state lolFor those of you who no longer prescribe any opiates, how did you get there?
What are your tips on doing so and how’s the best way to get there? What challenges are there to expect? Pitfalls?
For those of you who no longer prescribe any opiates, how did you get there?
What are your tips on doing so and how’s the best way to get there? What challenges are there to expect? Pitfalls?
#5 wut?1. Do not take over opioids and do not use Pain in your Name / logo
2. Explain to the patient and referring physicians that opioids are the last resort, explain multidisciplinary approach, opioid crisis, coping mechanism, home exercise program, pT, Chiro, non opioid meds, interventional procedures, psych referrals.
3. If you have a non opioid practise, then you should offer and facilitate a lot more than just injections
4. Your results will bring more patients.
5. And if someone needs opioids, prescribe.
1. Do not take over opioids and do not use Pain in your Name / logo
I agree not having pain in your name/logo or calling yourself as pain medicine or management doctor. I was once asked by PCP that you are pain medicine doctor but why you don't prescribe pain medicine (opioids)?"Interventional orthopedics" is gaining a lot of traction. "Sports & Spine" is also attractive. Once you get the reputation as being the "structured opioid refill clinic," "the CDC guideline clinic," or the "addiction/harm reduction" guy/gal in town you'll go to the grave with that reputation.
I agree not having pain in your name/logo or calling yourself as pain medicine or management doctor. I was once asked by PCP that you are pain medicine doctor but why you don't prescribe pain medicine (opioids)?
There are some patients who need opioids. Handful of them who have exhausted everything. Granny has had Multiple back surgeries, failed everything. If she needs 2 tranadol a day or even N 5/ 2 a day then. I will prescribe it. Opioid is one of the tools in your box that should be used when appropriate.#5 wut?
I do if I think it’s part of their pain problem, maintaining unhealthy coping strategies, if they are on an unsafe combination of meds, or it is harmful for their comorbidities (OSA, cognitive decline, etc).Do you advise patient to get off opioids even when you are not the prescribing physician?
U see them monthly?There are some patients who need opioids. Handful of them who have exhausted everything. Granny has had Multiple back surgeries, failed everything. If she needs 2 tranadol a day or even N 5/ 2 a day then. I will prescribe it. Opioid is one of the tools in your box that should be used when appropriate.
You can give an add in the local newspaper clearly stating it like I do. Some will like it, some hate it. But you will do the right thing for yourself, your patients and your profession. And sleep well.
This board is now leaning worse than PROP.
Responsible Opioid Prescribing.
https://gizmodo.com/doctors-are-prescribing-fewer-opioids-but-not-always-f-1833264138
Sound like a bunch of whiny interventional radiologists.
Anyone look at their ACGME certificates? Mine say Physical Medicine and Rehabilitation and the other says Pain Medicine.
The scientific and medical arguments for the continued use of opioids are sparse in the absence of any significant number of high quality studies published that demonstrate 1. opioids are safer than other alternatives for chronic non-malignant pain and 2. opioids are effective in the treatment of chronic non-malignant pain. Family physicians in particular, continue to stupidly start patients on long term opioids because they confuse nociceptive acute pain with the neurological disease of chronic pain, they are ill equipped with alternatives, and they cave to patients demands/whines about how much it hurts. There is little thought given to long term consequences of permanent neurological changes induced by opioids given long term, the sequelae of increased falls/fractures/depression/sedation/DUI/death/iatrogenic opioid dependency not to mention legal risks, both civil and criminal. Pain physicians indeed are left to mop up after abandonment of fundamental principles of medicine by PCPs.
As much as I have misgivings about PROP, they have worked to move the pendulum of dosing appropriateness. There is little argument that very high dose (MED>200mg/day) are inappropriate for nearly 100% of chronic non-malignant pain patients. There are only a few patients for which high dose (MED>100mg/day) are ever appropriate in the same patient population. These high doses used to be seen in a significant percentage of the chronic pain population. Now the arguments are more focused towards the appropriateness/inappropriateness of moderate dosage opioids or low dose opioids long term for chronic non-malignant pain. We have few long term studies to support even these doses.
Doctors that continue prescribing very high or high dose opioids are standing on very shaky medical, scientific and legal grounds. Given the high percentage of pain physicians that have received threats of violence, licensure issues, civil litigation risks, and DEA scrutiny some practices are converting to non-opioid. Non-opioid practices have to find other ways to survive other than being the dumping ground for PCPs that are nervous or have been arrested for prescribing opioids inappropriately.
Currently the lens of the public and news organizations is focused on the mercenary practices of pharmaceutical manufacturers of opioids, but should that lens becomes focused on the prescribing physicians who lack the science behind justifying prescribing opioids for chronic non-malignant pain, we will see civil litigation/malpractice suits skyrocket. Physicians will be held as pariahs for ignoring 150 years of medical literature that warned of the consequences of freely prescribing opioids. Then it will be a race to the bottom, when zero opioid prescribing will not protect physicians from their past prescribing practices.
Is there any high quality literature supporting long-term functional improvement with opioids, in those patients who “really need it”? (Not asking to be sarcastic - I’m genuinely curious what’s out there to support opioid prescribing)PROP's ideology/ideas are disputed. Disputed ideology is not a basis for public policy. They are making political arguments.
NOIs there any high quality literature supporting long-term functional improvement with opioids, in those patients who “really need it”? (Not asking to be sarcastic - I’m genuinely curious what’s out there to support opioid prescribing)
Is there any high quality literature supporting long-term functional improvement with opioids, in those patients who “really need it”? (Not asking to be sarcastic - I’m genuinely curious what’s out there to support opioid prescribing)
If hospital administrator/employer wants you to RX opioids, tell them to go to f*cking medical school.
I just opened a practice right out of fellowship this past fall. Part of the reason I went on my own is because I wanted to build a “non opioid” based practice.
I started by introducing myself to the pcp’s in the community. I made it clear I wasn’t going to take over prescriptions. Initially this didn’t go over to well. My strategy coming in was to focus on prevention. I simply asked if they even thought about starting a patient on opioids, consult me first. Let me deal with it.
When patients would call to schedule an appointment my staff was trained to be upfront and clear. No opioid prescription will be written in our practice. This weeds out many drug seeking patients. I don’t wanna waste their time or mine. We have been lucky to create an atmosphere that is pleasant and our patients want to be a part of our clinic.
Over the last few months, my practice has evolved. In the beginning I was strict no opioids. Didn’t write my first script until January. As I developed a Rapport with patients and esp (the elderly, multiple surgeons, injections all previously failed) I started prescribing at every low doses. Currently I prescribe tramadol( no more then Bid) or at most norco ( 5/325 BID). I would say this is <1% of my practice.
I saw 36 new patients in January, 40 in February, and will have seen about 50-60 new patients this month.
Moral of my personal story is, stick with what you believe in but be willing to evolve. I would say I am in a fairly competitive area( 5 pain doctors in a rural community. I’m the only one that does “ no opioids”.
The scientific and medical arguments for the continued use of opioids are sparse in the absence of any significant number of high quality studies published that demonstrate 1. opioids are safer than other alternatives for chronic non-malignant pain and 2. opioids are effective in the treatment of chronic non-malignant pain. Family physicians in particular, continue to stupidly start patients on long term opioids because they confuse nociceptive acute pain with the neurological disease of chronic pain, they are ill equipped with alternatives, and they cave to patients demands/whines about how much it hurts. There is little thought given to long term consequences of permanent neurological changes induced by opioids given long term, the sequelae of increased falls/fractures/depression/sedation/DUI/death/iatrogenic opioid dependency not to mention legal risks, both civil and criminal. Pain physicians indeed are left to mop up after abandonment of fundamental principles of medicine by PCPs.
As much as I have misgivings about PROP, they have worked to move the pendulum of dosing appropriateness. There is little argument that very high dose (MED>200mg/day) are inappropriate for nearly 100% of chronic non-malignant pain patients. There are only a few patients for which high dose (MED>100mg/day) are ever appropriate in the same patient population. These high doses used to be seen in a significant percentage of the chronic pain population. Now the arguments are more focused towards the appropriateness/inappropriateness of moderate dosage opioids or low dose opioids long term for chronic non-malignant pain. We have few long term studies to support even these doses.
Doctors that continue prescribing very high or high dose opioids are standing on very shaky medical, scientific and legal grounds. Given the high percentage of pain physicians that have received threats of violence, licensure issues, civil litigation risks, and DEA scrutiny some practices are converting to non-opioid. Non-opioid practices have to find other ways to survive other than being the dumping ground for PCPs that are nervous or have been arrested for prescribing opioids inappropriately.
Currently the lens of the public and news organizations is focused on the mercenary practices of pharmaceutical manufacturers of opioids, but should that lens becomes focused on the prescribing physicians who lack the science behind justifying prescribing opioids for chronic non-malignant pain, we will see civil litigation/malpractice suits skyrocket. Physicians will be held as pariahs for ignoring 150 years of medical literature that warned of the consequences of freely prescribing opioids. Then it will be a race to the bottom, when zero opioid prescribing will not protect physicians from their past prescribing practices.
I just opened a practice right out of fellowship this past fall. Part of the reason I went on my own is because I wanted to build a “non opioid” based practice.
I started by introducing myself to the pcp’s in the community. I made it clear I wasn’t going to take over prescriptions. Initially this didn’t go over to well. My strategy coming in was to focus on prevention. I simply asked if they even thought about starting a patient on opioids, consult me first. Let me deal with it.
When patients would call to schedule an appointment my staff was trained to be upfront and clear. No opioid prescription will be written in our practice. This weeds out many drug seeking patients. I don’t wanna waste their time or mine. We have been lucky to create an atmosphere that is pleasant and our patients want to be a part of our clinic.
Over the last few months, my practice has evolved. In the beginning I was strict no opioids. Didn’t write my first script until January. As I developed a Rapport with patients and esp (the elderly, multiple surgeons, injections all previously failed) I started prescribing at every low doses. Currently I prescribe tramadol( no more then Bid) or at most norco ( 5/325 BID). I would say this is <1% of my practice.
I saw 36 new patients in January, 40 in February, and will have seen about 50-60 new patients this month.
Moral of my personal story is, stick with what you believe in but be willing to evolve. I would say I am in a fairly competitive area( 5 pain doctors in a rural community. I’m the only one that does “ no opioids”.
Funny, I did a pubmed search and that was the first relevant article I came across too. Impact on functionality score was not statistically significant (though just barely - p=.055 or so) and - third of the treatment group dropped out due to side effects.A 6-months, randomised, placebo-controlled evaluation of efficacy and tolerability of a low-dose 7-day buprenorphine transdermal patch in osteoarth... - PubMed - NCBI
"Implications A low dose 7-days buprenorphine patch at 5-20 μg/h is a possible means of pain relief in about 2/3 of elderly osteoarthritis patients, in whom pain is opioid-sensitive, surgery is not possible, NSAIDs and coxibs are not recommended, and paracetamol in tolerable doses is not effective enough. Vigilant focus on and management of opioid side effects are essential."
For 2-3 months initially, thenQ2 monthsU see them monthly?
😉Here is the final version
Render the patient insensate!I think it helps to not be anesthesiology trained as there seems to be an expectation that anesthesia trained pain doctors must manage medications.
While I agree with minimizing opioids when possible, I do prescribe and continue them.
I do see how it would simplify my life though, but I'm not ready to go there yet.
Why should you have "0 Opiates" as an absolute rule? Why can't you just use your judgement?
(Honestly asking)
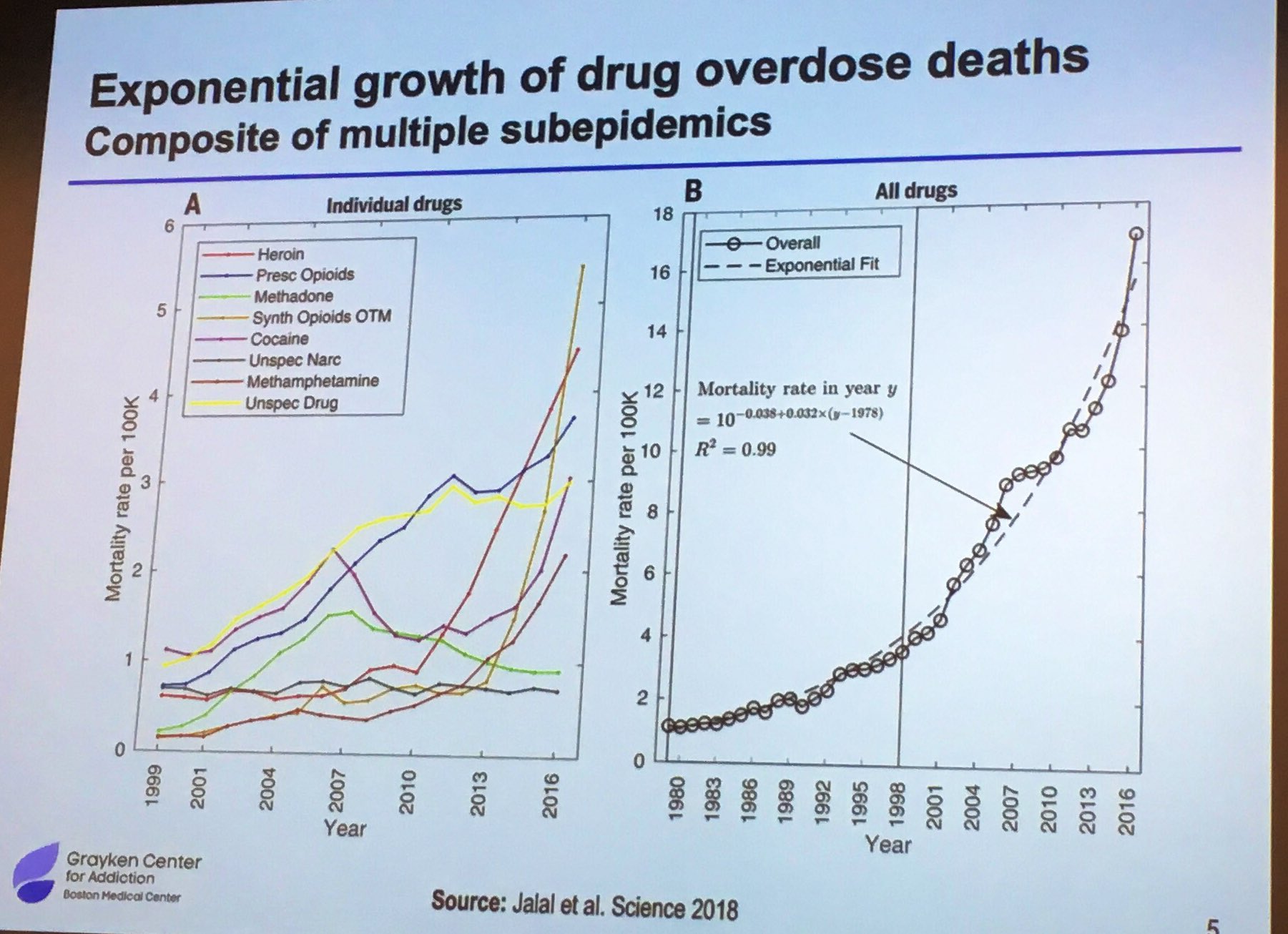
Changing dynamics of the drug overdose epidemic in the United States from 1979 through 2016Extremely interesting! What's really changed though? More prescriptions written or have patients gotten less responsible?